

Higher Dose Anticoagulation Cannot Prevent Disease Progression in COVID-19 Patients: A Systematic Review and Meta-Analysis
- PMID: 36140295
- PMCID: PMC9496532
- DOI: 10.3390/biomedicines10092194
Higher Dose Anticoagulation Cannot Prevent Disease Progression in COVID-19 Patients: A Systematic Review and Meta-Analysis
Abstract
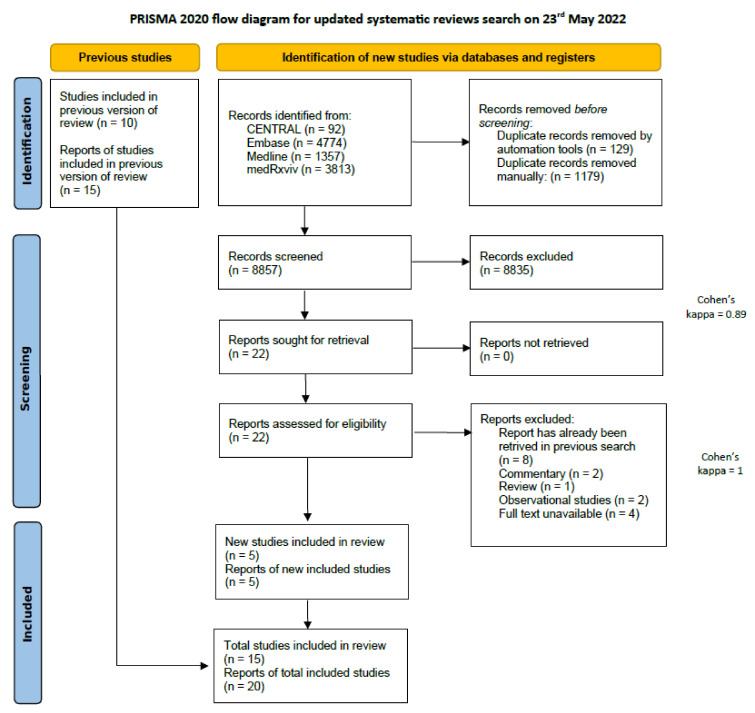
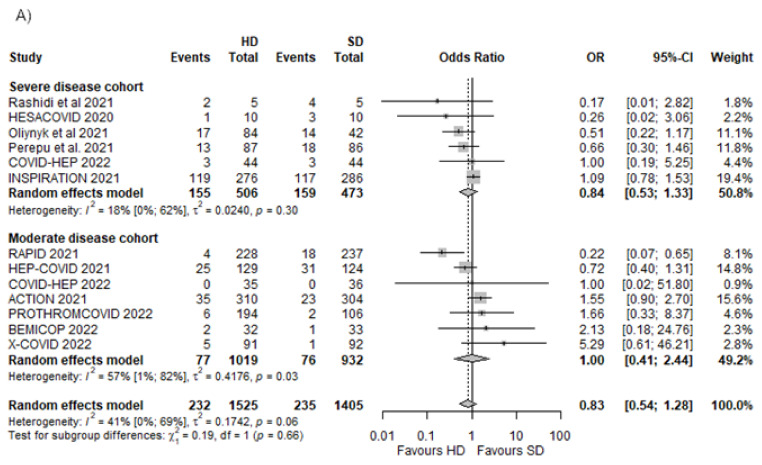
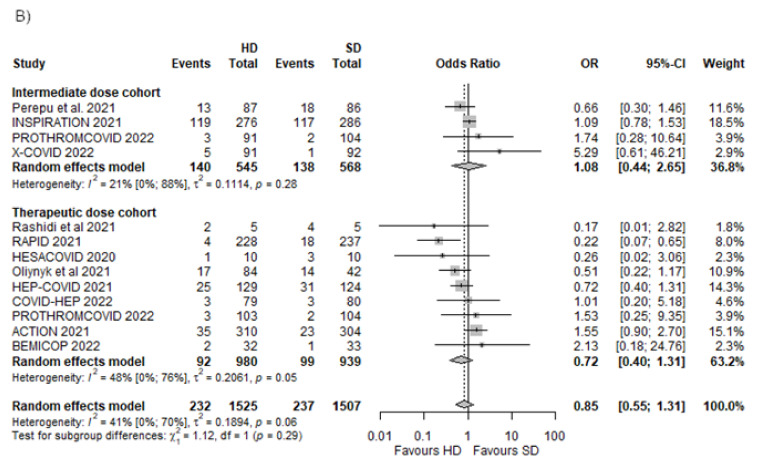
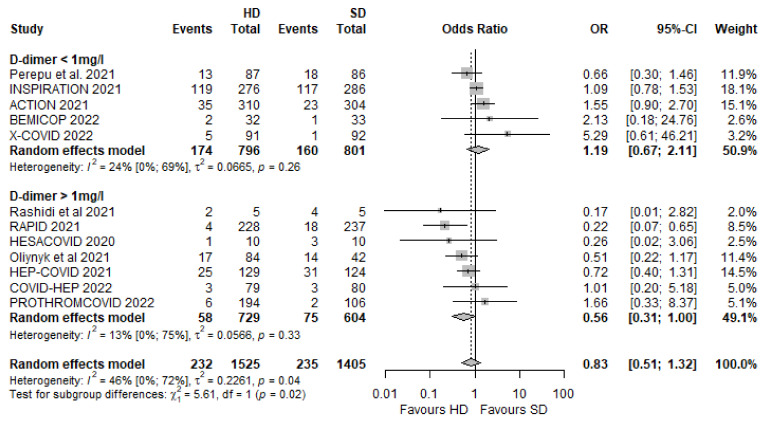
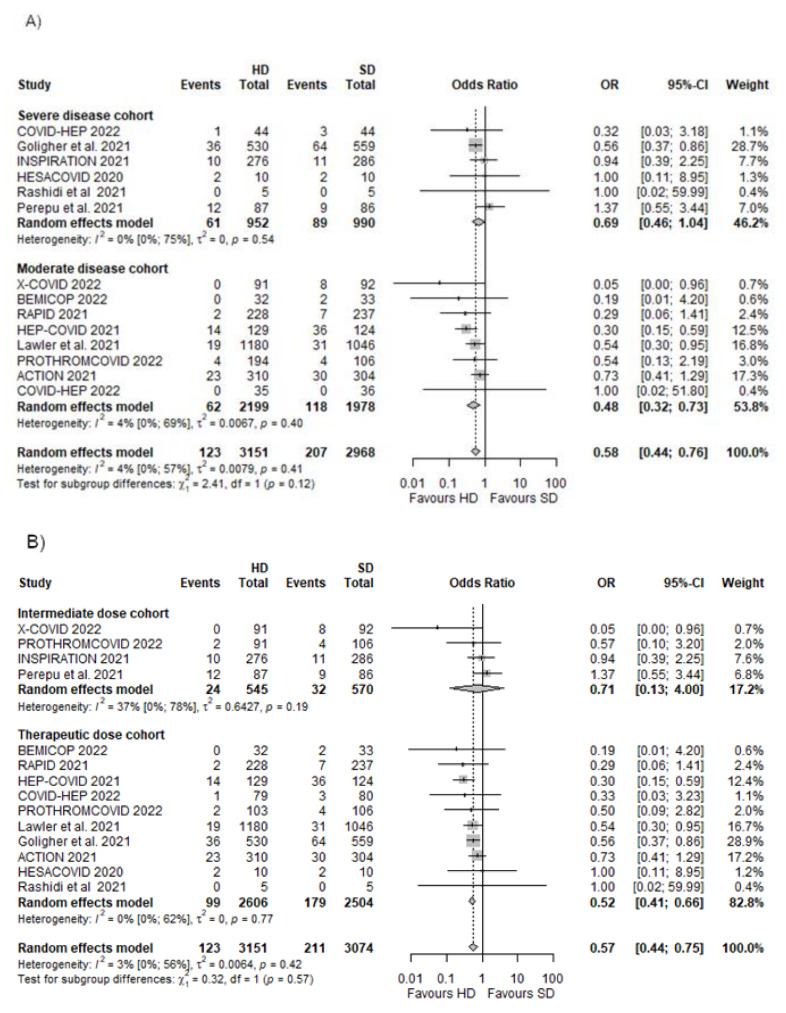
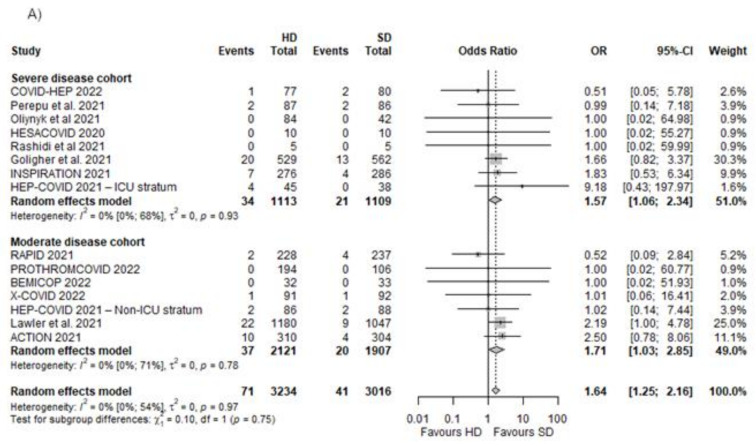
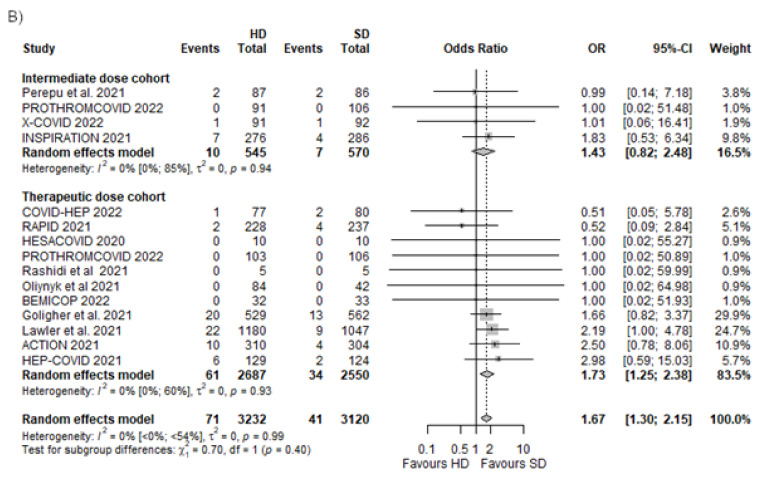
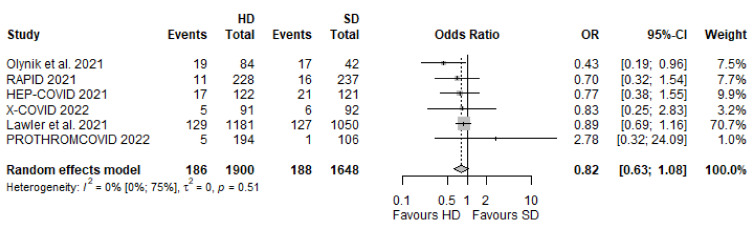
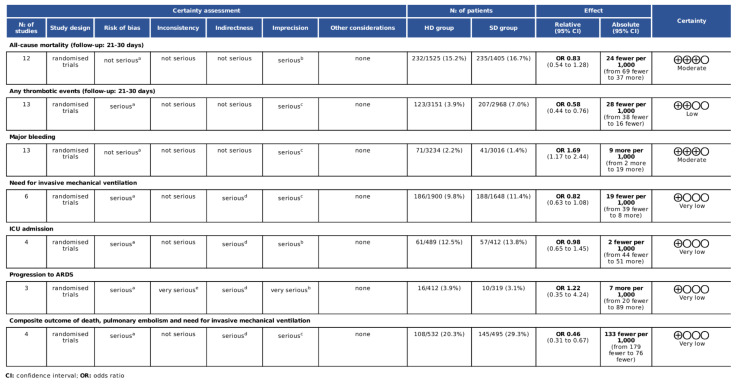
Implementation of higher dose (HD) thromboprophylaxis has been considered in patients infected with coronavirus disease 2019 (COVID-19). Our aim was to compare HD to standard dose (SD) thromboprophylaxis in COVID-19 patients. The protocol is registered on PROSPERO (CRD42021284808). We searched for randomised controlled studies (CENTRAL, Embase, Medline and medRxviv) that compared HD to SD anticoagulation in COVID-19 and analysed outcomes such as mortality, thrombotic events, bleedings, and disease progression. The statistical analyses were made using the random effects model. Fourteen articles were included (6253 patients). HD compared with SD showed no difference in mortality (OR 0.83 [95% CI 0.54−1.28]). The use of HD was associated with a decreased risk of thrombosis (OR 0.58 [95% CI 0.44−0.76]), although with an increased risk of major bleeding (OR 1.64 [95% CI 1.25−2.16]). The cohort with D-dimer < 1 mg/mL showed no effect (OR 1.19 [95% CI 0.67−2.11]), but in the case of D-dimer > 1 mg/mL, a tendency of lower risk in the HD group was observed (OR 0.56 [95% CI 0.31−1.00]). The need for intubation in moderately ill patients showed a nonsignificant lower likelihood in the HD group (OR 0.82 [95% CI 0.63−1.08]). We cannot advocate for HD in all COVID-19 patients, although it shows some nonsignificant benefits on disease progression in those with elevated D-dimer who do not need ICU admission.
Keywords: COVID-19; anticoagulation; disease progression; thromboinflamation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Worldometer Worldometers.info. 2022. [(accessed on 30 July 2022)]. Available online: https://www.worldometers.info/coronavirus/
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
