

Reduced Quality of Life in Patients with Non-Alcoholic Fatty Liver Disease May Be Associated with Depression and Fatigue
- PMID: 36141310
- PMCID: PMC9498740
- DOI: 10.3390/healthcare10091699
Reduced Quality of Life in Patients with Non-Alcoholic Fatty Liver Disease May Be Associated with Depression and Fatigue
Abstract
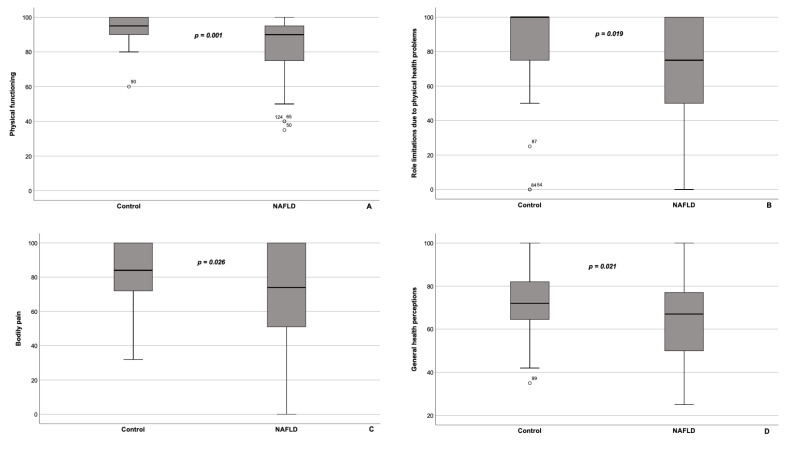
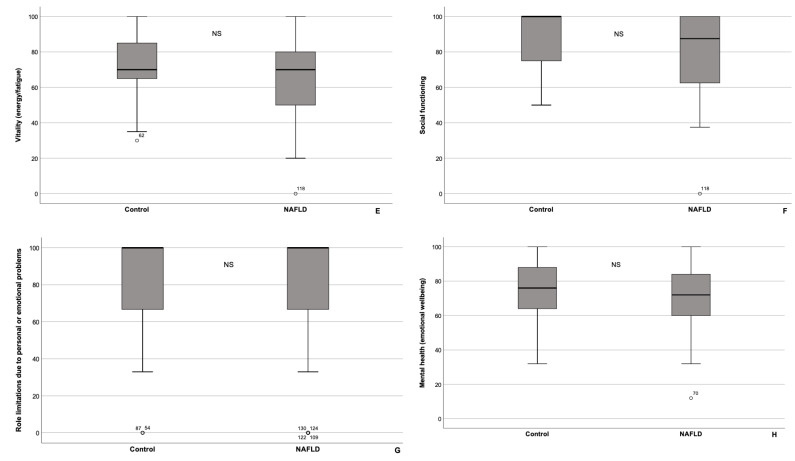
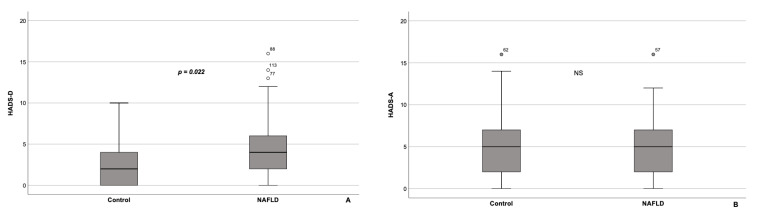
Non-alcoholic fatty liver disease (NAFLD) is often thought of as clinically asymptomatic. However, many NAFLD patients complain of fatigue and low mood, which may affect their quality of life (QoL). This may create a barrier to weight loss and hinder the achievement of NAFLD therapy goals. Our study aimed to evaluate the QoL in NAFLD patients vs. healthy volunteers, and to analyze likely influencing factors. From March 2021 through December 2021, we enrolled 140 consecutive adult subjects (100 NAFLD patients and 40 controls). Overall, 95 patients with NAFLD and 37 controls were included in the final analysis. Fatty liver was diagnosed based on ultrasonographic findings. We employed 36-Item Short Form Health Survey (SF-36) to evaluate QoL, Hospital Anxiety and Depression Scale (HADS) to identify anxiety and/or depression, and Fatigue Assessment Scale (FAS) to measure fatigue. NAFLD patients had significantly lower physical component summary scores, as well as significantly higher HADS-D scores, compared with the control group (Mann-Whitney U criterion = 1140.0, p = 0.001 and U = 1294.5, p = 0.022, respectively). Likewise, fatigue was more common in NAFLD patients (χ2 = 4.008, p = 0.045). Impaired QoL was significantly associated with fatigue (FAS score ≥ 22, p < 0.001) and depression (HADS-D ≥ 8, p < 0.001). In conclusion, NAFLD patients had significantly poorer QoL vs. controls, in particular with respect to the physical component of health. Impaired QoL may be associated with fatigue and depression, and together they may interfere with increased physical activity and lifestyle modifications in patients with NAFLD.
Keywords: SF-36; depression; fatigue; lifestyle modifications; non-alcoholic fatty liver disease; quality of life.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Clinically Meaningful Fatigue and Depression Are Associated with Sarcopenia in Patients with Non-Alcoholic Fatty Liver Disease.J Pers Med. 2023 May 31;13(6):932. doi: 10.3390/jpm13060932. J Pers Med. 2023. PMID: 37373921 Free PMC article.
-
Fatigue in patients with Behçet's syndrome: relationship with quality of life, depression, anxiety, disability and disease activity.Int J Rheum Dis. 2018 Dec;21(12):2139-2145. doi: 10.1111/1756-185X.12839. Epub 2016 Feb 23. Int J Rheum Dis. 2018. PMID: 26913703
-
The effect of polypharmacy on quality of life in adult patients with nonalcoholic fatty liver disease in the United States.Qual Life Res. 2022 Aug;31(8):2481-2491. doi: 10.1007/s11136-022-03090-6. Epub 2022 Jan 22. Qual Life Res. 2022. PMID: 35064417
-
Patient-reported outcomes in patients with non-alcoholic fatty liver disease: A narrative review of Chronic Liver Disease Questionnaire-non-alcoholic fatty liver disease/non-alcoholic steatohepatitis.J Gastroenterol Hepatol. 2021 Mar;36(3):629-636. doi: 10.1111/jgh.15172. Epub 2020 Jul 16. J Gastroenterol Hepatol. 2021. PMID: 32627871 Review.
-
Nonalcoholic fatty liver disease: lifestyle and quality of life.Hormones (Athens). 2022 Mar;21(1):41-49. doi: 10.1007/s42000-021-00339-6. Epub 2021 Dec 1. Hormones (Athens). 2022. PMID: 34854066 Review.
Cited by
-
Clinically Meaningful Fatigue and Depression Are Associated with Sarcopenia in Patients with Non-Alcoholic Fatty Liver Disease.J Pers Med. 2023 May 31;13(6):932. doi: 10.3390/jpm13060932. J Pers Med. 2023. PMID: 37373921 Free PMC article.
-
Mobile App-Based Lifestyle Coaching Intervention for Patients With Nonalcoholic Fatty Liver Disease: Randomized Controlled Trial.J Med Internet Res. 2024 Feb 15;26:e49839. doi: 10.2196/49839. J Med Internet Res. 2024. PMID: 38358794 Free PMC article. Clinical Trial.
-
Tryptophan Prevents the Development of Non-Alcoholic Fatty Liver Disease.Diabetes Metab Syndr Obes. 2023 Dec 23;16:4195-4204. doi: 10.2147/DMSO.S444278. eCollection 2023. Diabetes Metab Syndr Obes. 2023. PMID: 38152280 Free PMC article.
-
Rate and Associated Factors of Fatigue in Chinese Patients with Non-Alcoholic Fatty Liver Disease: A Cross-Sectional Survey.Int J Gen Med. 2024 Jul 4;17:2945-2953. doi: 10.2147/IJGM.S466980. eCollection 2024. Int J Gen Med. 2024. PMID: 38984071 Free PMC article.
-
MASLD: Prevalence, Mechanisms, and Sex-Based Therapies in Postmenopausal Women.Biomedicines. 2025 Apr 2;13(4):855. doi: 10.3390/biomedicines13040855. Biomedicines. 2025. PMID: 40299427 Free PMC article. Review.
References
-
- Finucane M.M., Stevens G.A., Cowan M.J., Danaei G., Lin J.K., Paciorek C.J., Singh G.M., Gutierrez H.R., Lu Y., Bahalim A.N., et al. Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Body Mass Index). National, regional, and global trends in body-mass index since 1980: Systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9·1 million participants. Lancet. 2011;377:557–567. doi: 10.1016/S0140-6736(10)62037-5. - DOI - PMC - PubMed
-
- Tomeno W., Kawashima K., Yoneda M., Saito S., Ogawa Y., Honda Y., Kessoku T., Imajo K., Mawatari H., Fujita K., et al. Non-alcoholic fatty liver disease comorbid with major depressive disorder: The pathological features and poor therapeutic efficacy. J. Gastroenterol. Hepatol. 2015;30:1009–1014. doi: 10.1111/jgh.12897. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
