

The Impact of Mouth-Taping in Mouth-Breathers with Mild Obstructive Sleep Apnea: A Preliminary Study
- PMID: 36141367
- PMCID: PMC9498537
- DOI: 10.3390/healthcare10091755
The Impact of Mouth-Taping in Mouth-Breathers with Mild Obstructive Sleep Apnea: A Preliminary Study
Abstract
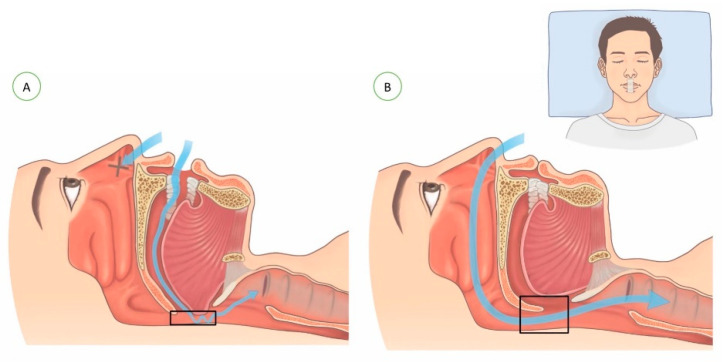
Background: Many patients with obstructive sleep apnea (OSA) are mouth-breathers. Mouth-breathing not only narrows the upper airway, consequently worsening the severity of OSA, but also it affects compliance with nasal continuous positive airway pressure (CPAP) treatment. This study aimed to investigate changes in OSA by the use of mouth tape in mouth-breathers with mild OSA.
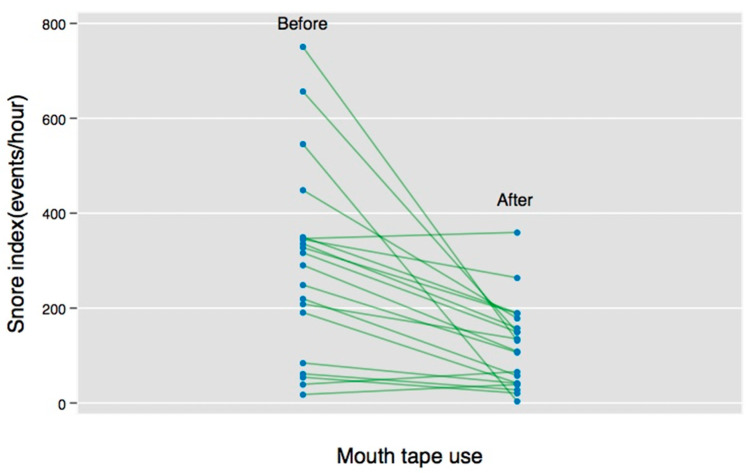
Method: Mouth-breathers with mild OSA who met inclusion criteria and tolerated the sealing of the mouth were enrolled in the study. We used 3M silicone hypoallergenic tape was used to seal the mouths of the participants during sleep. The home sleep test (HST) used in this study was ApneaLink®. Subjects received both a baseline HST and an outcome HST to be used 1 week later while their mouths were taped. The changes between the baseline and the outcome HSTs were compared, and the factors that influenced the differences in the sleep-test parameters after the shift of the breathing route were analyzed. A "responder" was defined as a patient who experienced a reduction from the baseline snoring index of at least 50% under mouth-taping in the HST; otherwise, patients were considered as having a poor response.
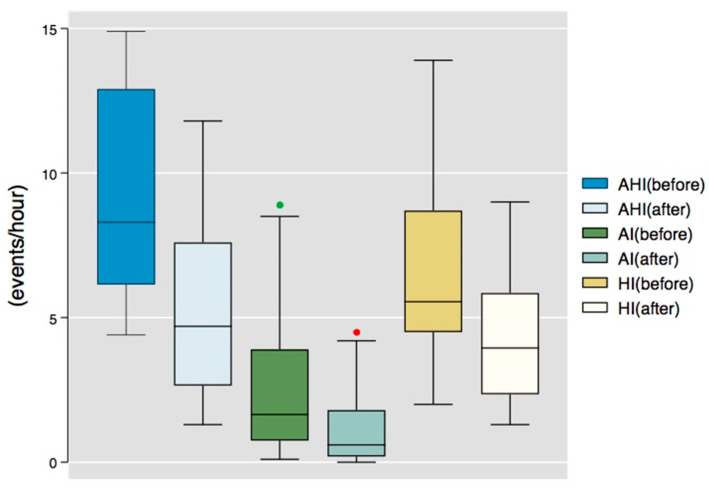
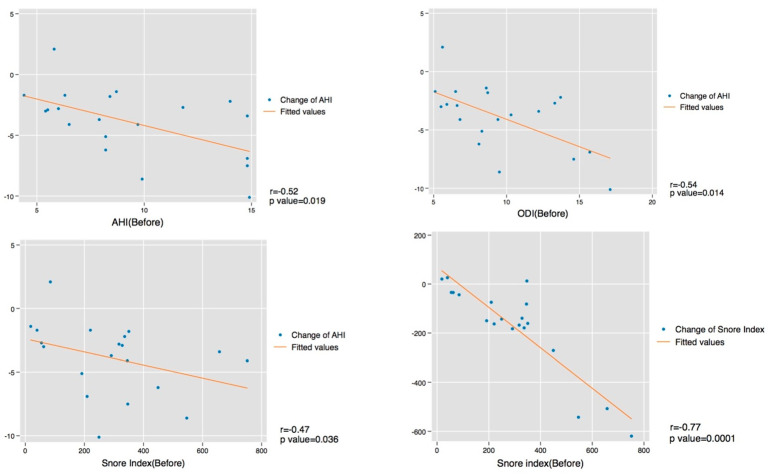
Results: A total of 20 patients with mild OSA were included. Following the taping of the mouth, a good response was found in 13 patients (65%). The median apnea/hypopnea index (AHI) decreased significantly, from 8.3 to 4.7 event/h (by 47%, p = 0.0002), especially in supine AHI (9.4 vs. 5.5 event/h, p = 0.0001). The median snoring index (SI) was also improved (by 47%, 303.8 vs. 121.1 event/h, p = 0.0002). Despite no significant difference in the mean saturation, improvements in the oxygen desaturation index (8.7 vs. 5.8, p = 0.0003) and the lowest saturation (82.5% vs. 87%, p = 0.049) were noted. The change in AHI was associated with baseline AHI (r = -0.52, p = 0.02), oxygen desaturation index (ODI) (r = -0.54, p = 0.01), and SI (r = -0.47, p = 0.04). The change in SI was strongly associated with baseline SI (r = -0.77, p = 0.001).
Conclusions: Mouth-taping during sleep improved snoring and the severity of sleep apnea in mouth-breathers with mild OSA, with AHI and SI being reduced by about half. The higher the level of baseline AHI and SI, the greater the improvement was shown after mouth-taping. Mouth-taping could be an alternative treatment in patients with mild OSA before turning to CPAP therapy or surgical intervention.
Keywords: mouth-breathing; mouth-taping; obstructive sleep apnea; snoring.
Conflict of interest statement
The named authors have no conflicts of interest, financial or otherwise.
Figures
References
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
