

Clinical Implications of the Genetic Background in Pediatric Pulmonary Arterial Hypertension: Data from the Spanish REHIPED Registry
- PMID: 36142358
- PMCID: PMC9499494
- DOI: 10.3390/ijms231810433
Clinical Implications of the Genetic Background in Pediatric Pulmonary Arterial Hypertension: Data from the Spanish REHIPED Registry
Abstract
Background: Pulmonary arterial hypertension (PAH) is a severe and rare disease with an important genetic background. The influence of genetic testing in the clinical classification of pediatric PAH is not well known and genetics could influence management and prognosis.
Objectives: The aim of this work was to identify the molecular fingerprint of PH children in the REgistro de pacientes con HIpertensión Pulmonar PEDiátrica (REHIPED), and to investigate if genetics could have an impact in clinical reclassification and prognosis.
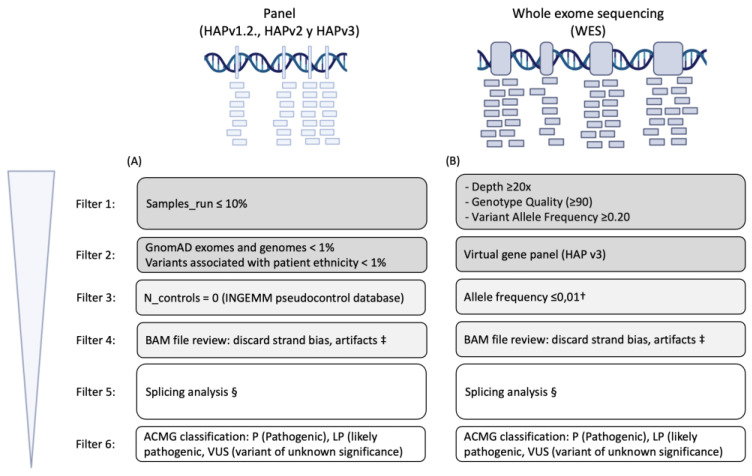
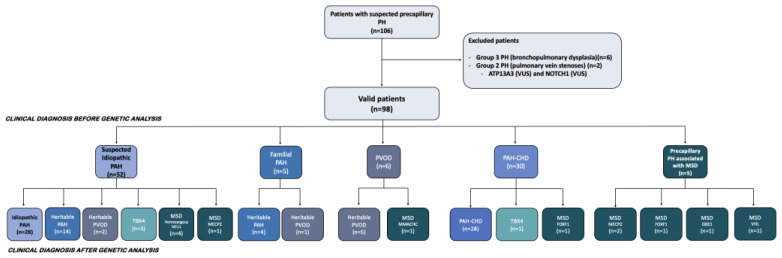
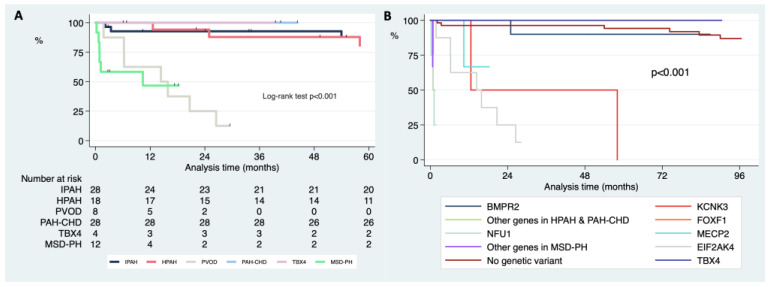
Methods: We included pediatric patients with a genetic analysis from REHIPED. From 2011 onward, successive genetic techniques have been carried out. Before genetic diagnosis, patients were classified according to their clinical and hemodynamic data in five groups. After genetic analysis, the patients were reclassified. The impact of genetics in survival free of lung transplantation was estimated by Kaplan-Meier curves.
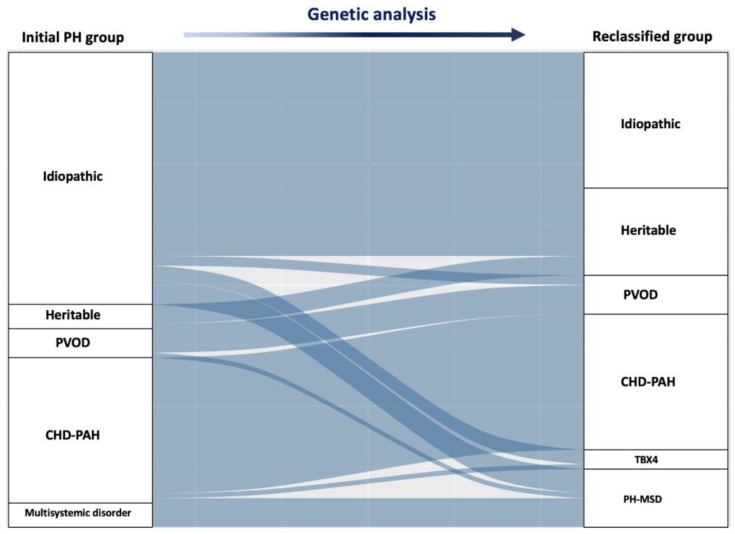
Results: Ninety-eight patients were included for the analysis. Before the genetic diagnoses, there were idiopathic PAH forms in 53.1%, PAH associated with congenital heart disease in 30.6%, pulmonary veno-occlusive disease-PVOD-in 6.1%, familial PAH in 5.1%, and associated forms with multisystemic disorders-MSD-in 5.1% of the patients. Pathogenic or likely pathogenic variants were found in 44 patients (44.9%). After a genetic analysis, 28.6% of the cohort was "reclassified", with the groups of heritable PAH, heritable PVOD, TBX4, and MSD increasing up to 18.4%, 8.2%, 4.1%, and 12.2%, respectively. The MSD forms had the worst survival rates, followed by PVOD.
Conclusions: Genetic testing changed the clinical classification of a significant proportion of patients. This reclassification showed relevant prognostic implications.
Keywords: genetics; heritable pulmonary arterial hypertension; pediatric pulmonary hypertension; pulmonary veno-occlusive disease.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Humbert M., Guignabert C., Bonnet S., Dorfmüller P., Klinger J.R., Nicolls M.R., Olschewski A.J., Pullamsetti S.S., Schermuly R.T., Stenmark K.R., et al. Pathology and pathobiology of pulmonary hypertension: State of the art and research perspectives. Eur. Respir. J. 2019;53:1801887. doi: 10.1183/13993003.01887-2018. - DOI - PMC - PubMed
-
- Cerro M.J., Abman S., Diaz G., Freudenthal A.H., Freudenthal F., Harikrishnan S., Haworth S.G., Ivy D., Lopes A.A., Raj J.U., et al. A consensus approach tothe classification of pediatric pulmonary hypertensive vascular disease: Report from the PVRI Pediatric Taskforce, Panama 2011. Pulm. Circ. 2011;1:286–298. doi: 10.4103/2045-8932.83456. - DOI - PMC - PubMed
