

Cold Atmospheric Plasma Jet Treatment Improves Human Keratinocyte Migration and Wound Closure Capacity without Causing Cellular Oxidative Stress
- PMID: 36142561
- PMCID: PMC9504313
- DOI: 10.3390/ijms231810650
Cold Atmospheric Plasma Jet Treatment Improves Human Keratinocyte Migration and Wound Closure Capacity without Causing Cellular Oxidative Stress
Abstract
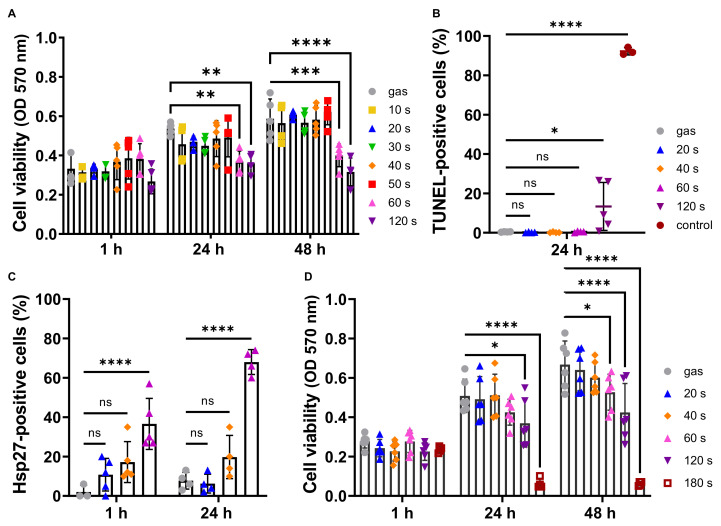
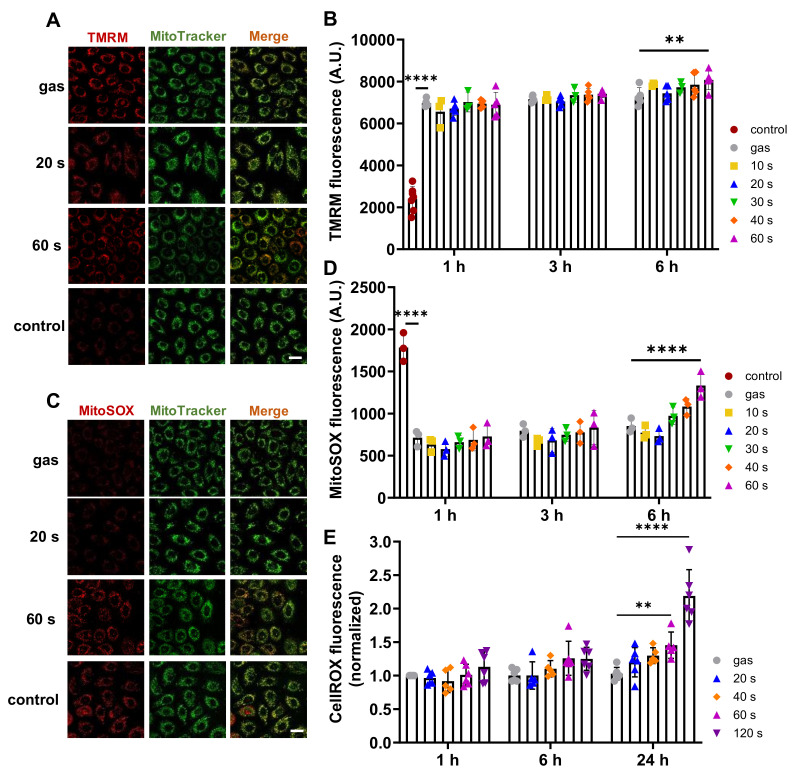
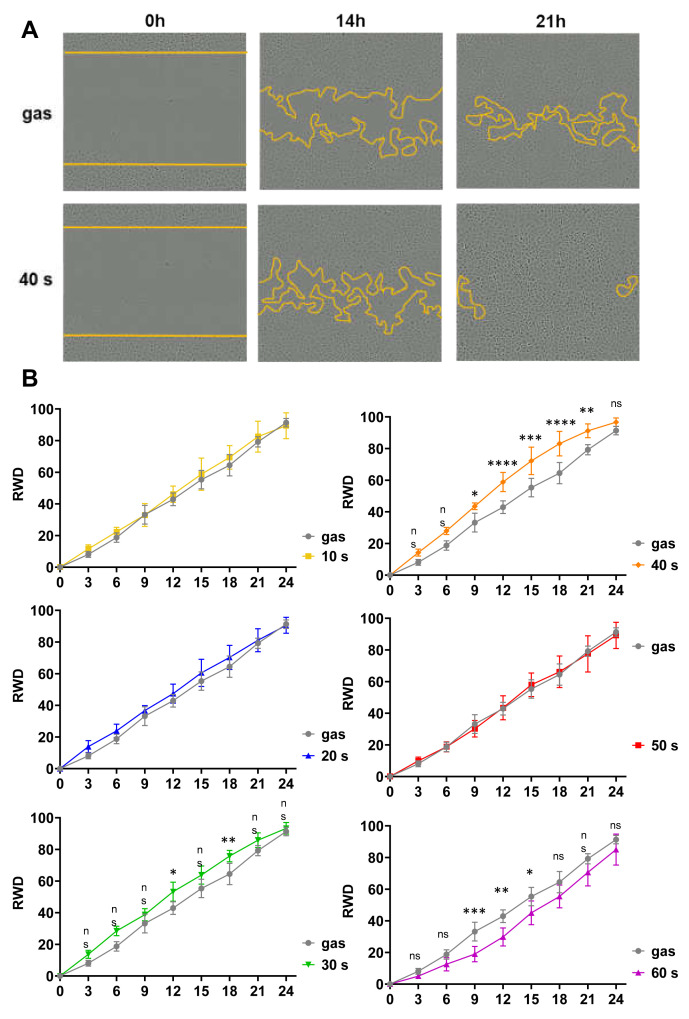
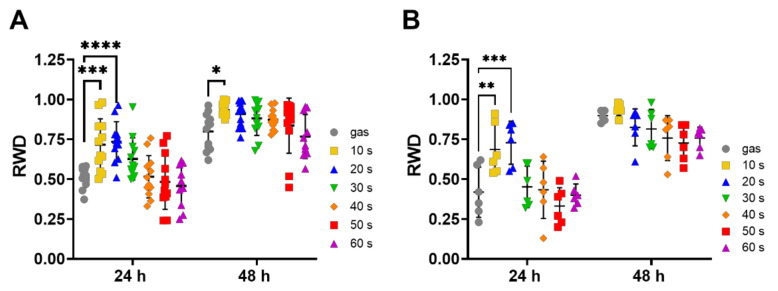
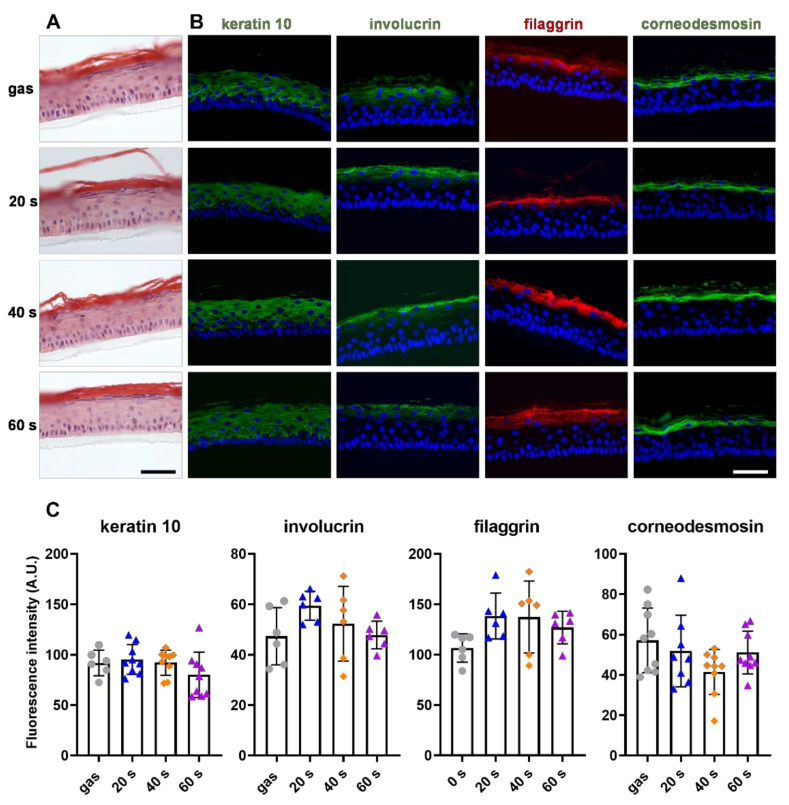
Cold Atmospheric Plasma (CAP) is an emerging technology with great potential for biomedical applications such as sterilizing equipment and antitumor strategies. CAP has also been shown to improve skin wound healing in vivo, but the biological mechanisms involved are not well known. Our study assessed a possible effect of a direct helium jet CAP treatment on keratinocytes, in both the immortalized N/TERT-1 human cell line and primary keratinocytes obtained from human skin samples. The cells were covered with 200 µL of phosphate buffered saline and exposed to the helium plasma jet for 10−120 s. In our experimental conditions, micromolar concentrations of hydrogen peroxide, nitrite and nitrate were produced. We showed that long-time CAP treatments (≥60 s) were cytotoxic, reduced keratinocyte migration, upregulated the expression of heat shock protein 27 (HSP27) and induced oxidative cell stress. In contrast, short-term CAP treatments (<60 s) were not cytotoxic, did not affect keratinocyte proliferation and differentiation, and did not induce any changes in mitochondria, but they did accelerate wound closure in vitro by improving keratinocyte migration. In conclusion, these results suggest that helium-based CAP treatments improve wound healing by stimulating keratinocyte migration. The study confirms that CAP could be a novel therapeutic method to treat recalcitrant wounds.
Keywords: cell migration; cold atmospheric plasma; keratinocytes; oxidative stress; reactive oxygen and nitrogen species; skin; wound healing.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Dunnill C., Patton T., Brennan J., Barrett J., Dryden M., Cooke J., Leaper D., Georgopoulos N.T. Reactive oxygen species (ROS) and wound healing: The functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int. Wound J. 2017;14:89–96. doi: 10.1111/iwj.12557. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
