

Recent Advances in the Emerging Therapeutic Strategies for Diabetic Kidney Diseases
- PMID: 36142794
- PMCID: PMC9506036
- DOI: 10.3390/ijms231810882
Recent Advances in the Emerging Therapeutic Strategies for Diabetic Kidney Diseases
Abstract
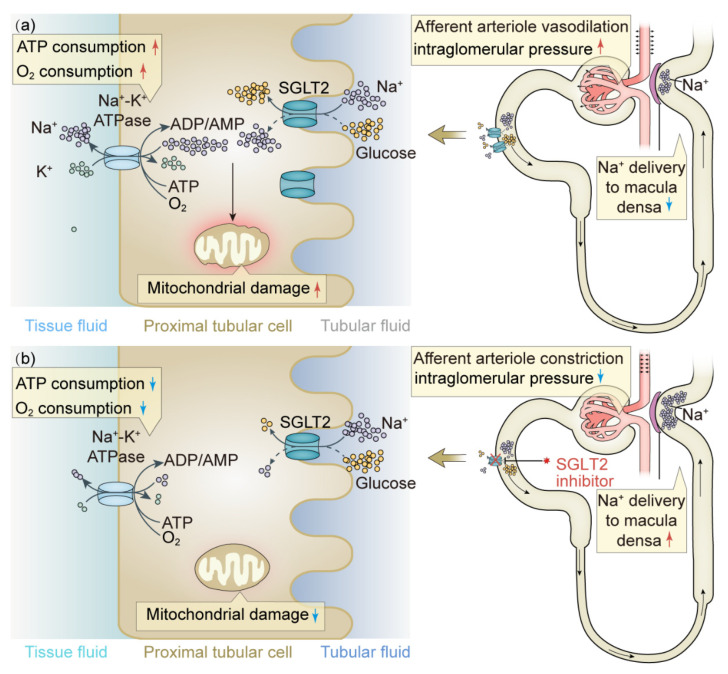
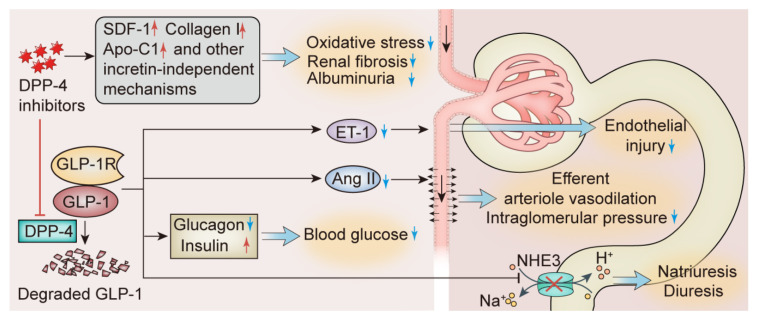
Diabetic kidney disease (DKD) is one of the most common causes of end-stage renal disease worldwide. The treatment of DKD is strongly associated with clinical outcomes in patients with diabetes mellitus. Traditional therapeutic strategies focus on the control of major risk factors, such as blood glucose, blood lipids, and blood pressure. Renin-angiotensin-aldosterone system inhibitors have been the main therapeutic measures in the past, but the emergence of sodium-glucose cotransporter 2 inhibitors, incretin mimetics, and endothelin-1 receptor antagonists has provided more options for the management of DKD. Simultaneously, with advances in research on the pathogenesis of DKD, some new therapies targeting renal inflammation, fibrosis, and oxidative stress have gradually entered clinical application. In addition, some recently discovered therapeutic targets and signaling pathways, mainly in preclinical and early clinical trial stages, are expected to provide benefits for patients with DKD in the future. This review summarizes the traditional treatments and emerging management options for DKD, demonstrating recent advances in the therapeutic strategies for DKD.
Keywords: SGLT2 inhibitors; diabetic kidney disease; fibrosis; inflammation; therapeutics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Pathophysiologic mechanisms in diabetic kidney disease: A focus on current and future therapeutic targets.Diabetes Obes Metab. 2020 Apr;22 Suppl 1:16-31. doi: 10.1111/dom.13969. Diabetes Obes Metab. 2020. PMID: 32267077 Review.
-
What's New in the Molecular Mechanisms of Diabetic Kidney Disease: Recent Advances.Int J Mol Sci. 2022 Dec 29;24(1):570. doi: 10.3390/ijms24010570. Int J Mol Sci. 2022. PMID: 36614011 Free PMC article. Review.
-
A Narrative Review of Diabetic Kidney Disease: Previous and Current Evidence-Based Therapeutic Approaches.Adv Ther. 2022 Aug;39(8):3488-3500. doi: 10.1007/s12325-022-02223-0. Epub 2022 Jun 25. Adv Ther. 2022. PMID: 35751762 Review.
-
Molecular Targets of Novel Therapeutics for Diabetic Kidney Disease: A New Era of Nephroprotection.Int J Mol Sci. 2024 Apr 3;25(7):3969. doi: 10.3390/ijms25073969. Int J Mol Sci. 2024. PMID: 38612779 Free PMC article. Review.
-
Recent advances in the pharmacotherapeutic management of diabetic kidney disease.Expert Opin Pharmacother. 2022 May;23(7):791-803. doi: 10.1080/14656566.2022.2054699. Epub 2022 May 6. Expert Opin Pharmacother. 2022. PMID: 35522659
Cited by
-
A Network Pharmacology-Based Investigation into the Mechanism of Quercetin Combined with Rosuvastatin in Delaying Diabetic Nephropathy via Inhibiting NRK-52E Cell Ferroptosis.Diabetes Metab Syndr Obes. 2025 Aug 5;18:2681-2694. doi: 10.2147/DMSO.S524983. eCollection 2025. Diabetes Metab Syndr Obes. 2025. PMID: 40785752 Free PMC article.
-
DNA methylation enzymes in the kidneys of male and female BTBR ob/ob mice.Front Endocrinol (Lausanne). 2023 Apr 5;14:1167546. doi: 10.3389/fendo.2023.1167546. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37091852 Free PMC article.
-
Resveratrol delays the progression of diabetic nephropathy through multiple pathways: A dose-response meta-analysis based on animal models.J Diabetes. 2024 Sep;16(9):e13608. doi: 10.1111/1753-0407.13608. J Diabetes. 2024. PMID: 39264004 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
