

The Small Posterior Cranial Fossa Syndrome and Chiari Malformation Type 0
- PMID: 36143119
- PMCID: PMC9503629
- DOI: 10.3390/jcm11185472
The Small Posterior Cranial Fossa Syndrome and Chiari Malformation Type 0
Abstract
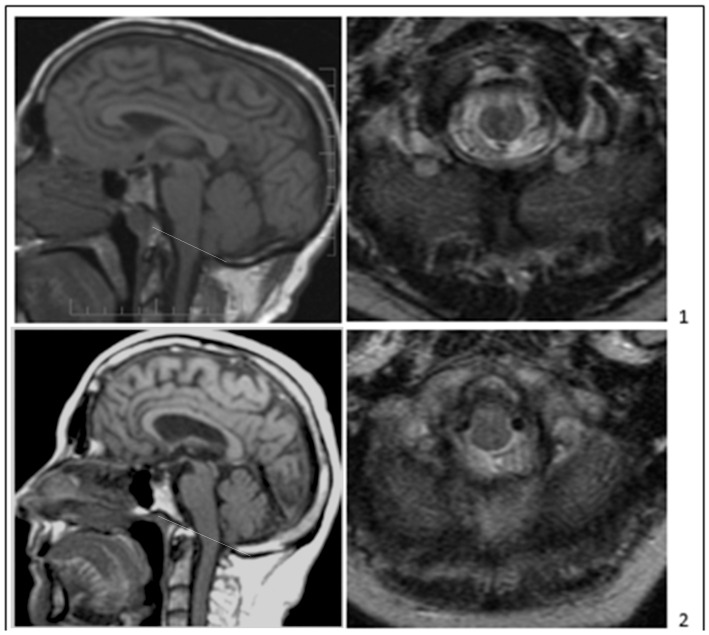
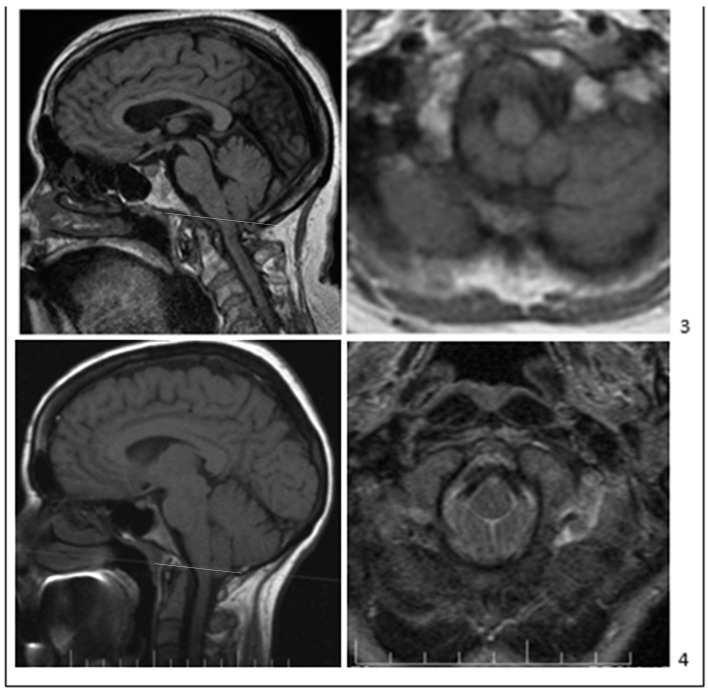
Patients showing typical Chiari malformation type 1 (CM1) signs and symptoms frequently undergo cranial and cervical MRI. In some patients, MRI documents >5 mm of cerebellar tonsillar herniation (TH) and the diagnosis of CM1. Patients with 3−5 mm TH have “borderline” CM1. Patients with less than 3 mm of TH and an associated cervical syrinx are diagnosed with Chiari “zero” malformation (CM0). However, patients reporting CM1 symptoms are usually not diagnosed with CM if MRI shows less than 3−5 mm of TH and no syrinx. Recent MRI morphometric analysis of the posterior fossa and upper cervical spine detected anatomical abnormalities in and around the foramen magnum (FM) that explain these patients’ symptoms. The abnormalities include a reduced size of the posterior fossa, FM, and upper cervical spinal canal and extension of the cerebellar tonsils around the medulla rather than inferior to the foramen magnum, as in CM1. These morphometric findings lead some neurologists and neurosurgeons to diagnose CM0 in patients with typical CM1 signs and symptoms, with or without cervical syringes. This article reviews recent findings and controversies about CM0 diagnosis and updates current thinking about the clinical and radiological relationship between CM0, borderline CM1, and CM1.
Keywords: Chiari malformation type 0; Chiari malformation type 1; cerebellar tonsil herniation; morphometric analysis; small posterior cranial fossa; syringomyelia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tubbs R.S., Turgut M. Defining the Chiari Malformations: Past and Newer Classifications. In: Tubbs R.S., Turgut M., Oakes W.J., editors. The Chiari Malformations. 2nd ed. Springer Nature Publishing; Cham, Switzerland: 2020. pp. 21–40.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
