

Comparison of the Post-Surgical Position of the Temporomandibular Joint after Orthognathic Surgery in Skeletal Class III Patients and Patients with Cleft Lip and Palate
- PMID: 36143222
- PMCID: PMC9506436
- DOI: 10.3390/jpm12091437
Comparison of the Post-Surgical Position of the Temporomandibular Joint after Orthognathic Surgery in Skeletal Class III Patients and Patients with Cleft Lip and Palate
Abstract
Objective: The purpose of our research is to compare the post-surgical position of the temporomandibular joint in skeletal Class III patients and patients with cleft lip and palate treated with two-jaw orthognathic surgery using a three-dimensional computer tomography image.
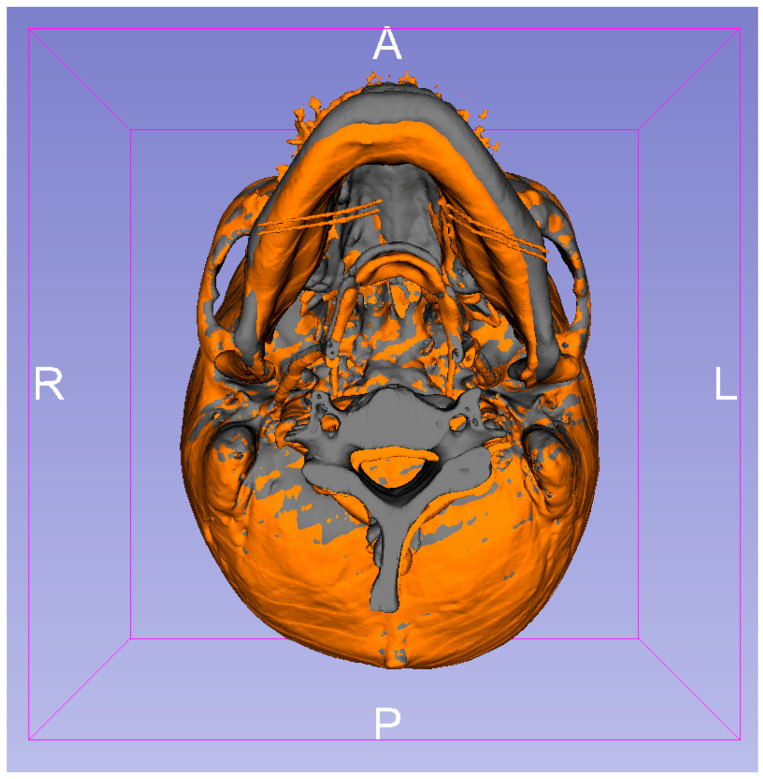
Materials and methods: Twenty-three skeletal Class III patients with mandibular prognathism associated with maxillary retrognathism in group 1 and twenty cleft mid-face retrusion skeletal Class III patients in group 2 were enrolled in this study. All subjects were treated with two-jaw orthognathic surgery. Computed tomography scans were taken in all subjects at 3 weeks preoperatively and 6 months postoperatively. Three-dimensional craniofacial skeletal structures were build-up, and assessed the temporomandibular joint position changes before and after surgery.
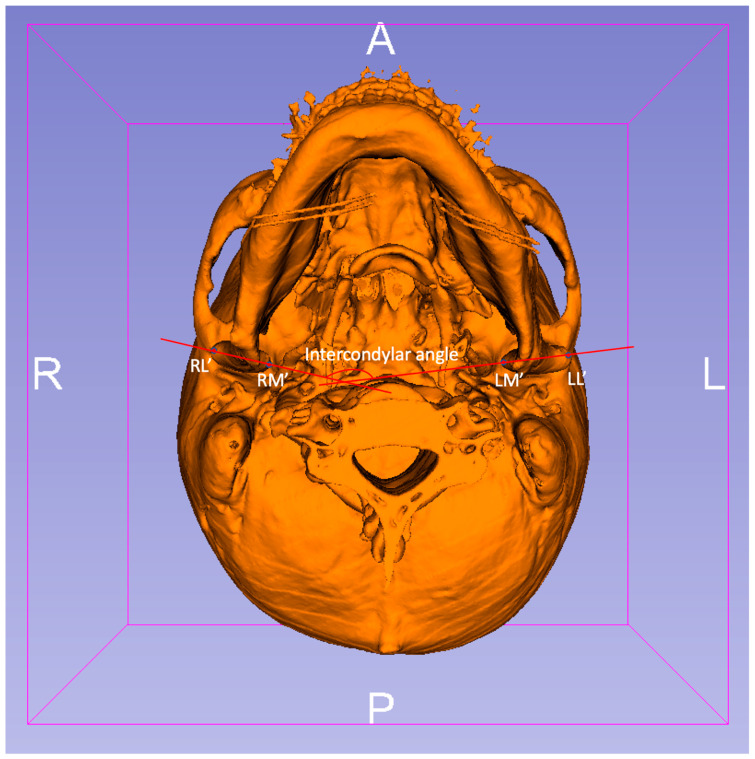
Results: Forty-three selected patients were separated into two groups. The mean age of patients was 22.39 ± 4.8 years in group 1 and 20.25 ± 3.8 years in group 2. The range of mean three-dimensional discrepancy of the selected condylar points was 0.95-1.23 mm in group 1 and 2.37-2.86 mm in group 2. The mean alteration of intercondylar angle was 2.33 ± 1.34° in group 1 and 6.30 ± 2.22° in group 2. The significant differences in the discrepancy of TMJ and changes in intercondylar angle were confirmed within the intra-group and between the two groups.
Conclusions: Significant changes in postoperative TMJ position were present in both groups. Furthermore, the cleft group presented significantly more postoperative discrepancy of TMJ and more changes in intercondylar angle after surgery. This finding may be a reason leading to greater postoperative instability in cleft patients compared with skeletal Class III non-cleft patients.
Clinical trial registration number: IRB No: 202201108B0.
Keywords: cleft lip and palate; computed tomography; orthognathic surgery; temporomandibular joint stability.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Hoppenreijs T.J., Freihofer H.P.M., Stoelinga P.J., Tuinzing D.B., van’t Hof M.A. Condylar remodelling and resorption after Le Fort I and bimaxillary osteotomies in patients with anterior open bite. A clinical and radiological study. Int. J. Oral Maxillofac. Surg. 1998;27:81–91. doi: 10.1016/S0901-5027(98)80301-9. - DOI - PubMed
-
- Sanromán J.F., Gonzalez J.G., Del Hoyo J.A., Gil F.M. Morphometric and morphological changes in the temporomandibular joint after orthognathic surgery: A magnetic resonance imaging and computed tomography prospective study. J. Cranio-Maxillofac. Surg. 1997;25:139–148. doi: 10.1016/S1010-5182(97)80005-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
