

Simultaneous Motor and Visual Intraoperative Neuromonitoring in Asleep Parietal Lobe Surgery: Dual Strip Technique
- PMID: 36143263
- PMCID: PMC9500827
- DOI: 10.3390/jpm12091478
Simultaneous Motor and Visual Intraoperative Neuromonitoring in Asleep Parietal Lobe Surgery: Dual Strip Technique
Abstract
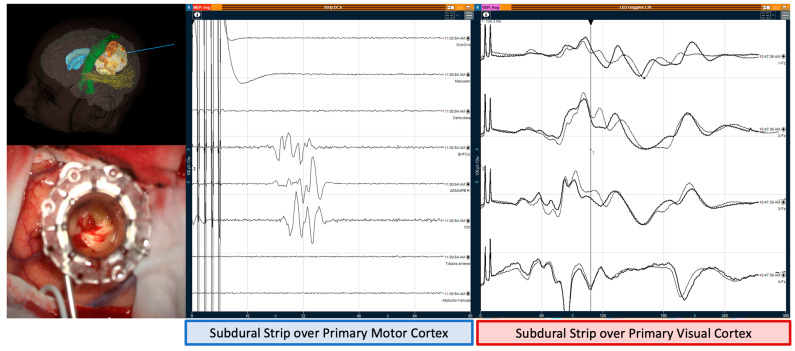
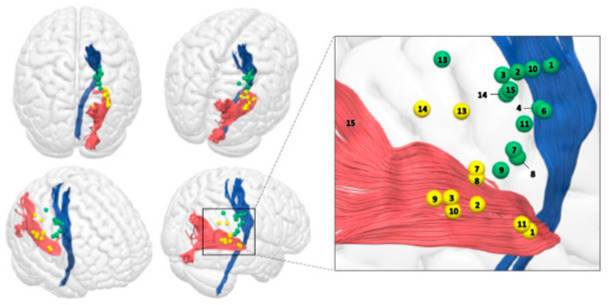
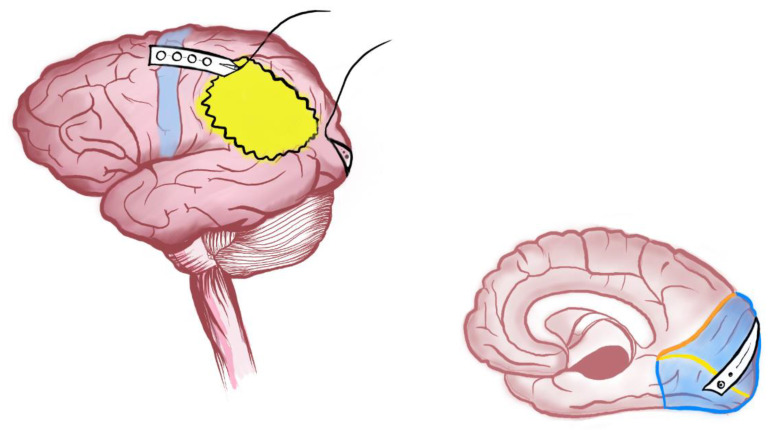
Background: The role played by the non-dominant parietal lobe in motor cognition, attention and spatial awareness networks has potentiated the use of awake surgery. When this is not feasible, asleep monitoring and mapping techniques should be used to achieve an onco-functional balance. Objective: This study aims to assess the feasibility of a dual-strip method to obtain direct cortical stimulation for continuous real-time cortical monitoring and subcortical mapping of motor and visual pathways simultaneously in parietal lobe tumour surgery. Methods: Single-centre prospective study between 19 May−20 November of patients with intrinsic non-dominant parietal-lobe tumours. Two subdural strips were used to simultaneously map and monitor motor and visual pathways. Results: Fifteen patients were included. With regards to motor function, a large proportion of patients had abnormal interhemispheric resting motor threshold ratio (iRMTr) (71.4%), abnormal Cortical Excitability Score (CES) (85.7%), close distance to the corticospinal tract—Lesion-To-Tract Distance (LTD)—4.2 mm, Cavity-To-Tract Distance (CTD)—7 mm and intraoperative subcortical distance—6.4 mm. Concerning visual function, the LTD and CTD for optic radiations (OR) were 0.5 mm and 3.4 mm, respectively; the mean intensity for positive subcortical stimulation of OR was 12 mA ± 2.3 mA and 5/6 patients with deterioration of VEPs > 50% had persistent hemianopia and transgression of ORs. Twelve patients remained stable, one patient had a de-novo transitory hemiparesis, and two showed improvements in motor symptoms. A higher iRMTr for lower limbs was related with a worse motor outcome (p = 0.013) and a longer CTD to OR was directly related with a better visual outcome (p = 0.041). At 2 weeks after hospital discharge, all patients were ambulatory at home, and all proceeded to have oncological treatment. Conclusion: We propose motor and visual function boundaries for asleep surgery of intrinsic non-dominant parietal tumours. Pre-operative abnormal cortical excitability of the motor cortex, deterioration of the VEP recordings and CTD < 2 mm from the OR were related to poorer outcomes.
Keywords: corticospinal tract; intra-operative neuro-monitoring; optic radiations; parietal lobe; subdural strip electrodes; tractography; transcranial magnetic stimulation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Intraoperative Neuromonitoring of the Visual Pathway in Asleep Neuro-Oncology Surgery.Cancers (Basel). 2023 Aug 3;15(15):3943. doi: 10.3390/cancers15153943. Cancers (Basel). 2023. PMID: 37568762 Free PMC article.
-
Elaborate mapping of the posterior visual pathway in awake craniotomy.J Neurosurg. 2018 May;128(5):1503-1511. doi: 10.3171/2017.2.JNS162757. Epub 2017 Aug 25. J Neurosurg. 2018. PMID: 28841121
-
Recording human electrocorticographic (ECoG) signals for neuroscientific research and real-time functional cortical mapping.J Vis Exp. 2012 Jun 26;(64):3993. doi: 10.3791/3993. J Vis Exp. 2012. PMID: 22782131 Free PMC article.
-
Intraoperative mapping and monitoring of the corticospinal tracts with neurophysiological assessment and 3-dimensional ultrasonography-based navigation. Clinical article.J Neurosurg. 2011 Mar;114(3):738-46. doi: 10.3171/2010.8.JNS10639. Epub 2010 Aug 27. J Neurosurg. 2011. PMID: 20799862
-
[Continuous monitoring of cortical visual evoked potentials by means of subdural electrodes in surgery on the posterior optic pathway. A case report and review of the literature].Rev Neurol. 2012 Sep 16;55(6):343-8. Rev Neurol. 2012. PMID: 22972576 Review. Spanish.
Cited by
-
Intraoperative Neurophysiological Monitoring in Neurosurgery.J Clin Med. 2024 May 17;13(10):2966. doi: 10.3390/jcm13102966. J Clin Med. 2024. PMID: 38792507 Free PMC article. Review.
References
-
- Lavrador J.P., Ghimire P., Brogna C., Furlanetti L., Patel S., Gullan R., Ashkan K., Bhangoo R., Vergani F. Pre- and Intraoperative Mapping for Tumors in the Primary Motor Cortex: Decision-Making Process in Surgical Resection. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2021;82:333–343. doi: 10.1055/s-0040-1709729. - DOI - PubMed
-
- Freund H.J. Somatosensory and motor disturbances in patients with parietal lobe lesions. Adv. Neurol. 2003;93:179–193. - PubMed
LinkOut - more resources
Full Text Sources
