

C3a and C5b-9 Differentially Predict COVID-19 Progression and Outcome
- PMID: 36143371
- PMCID: PMC9504647
- DOI: 10.3390/life12091335
C3a and C5b-9 Differentially Predict COVID-19 Progression and Outcome
Abstract
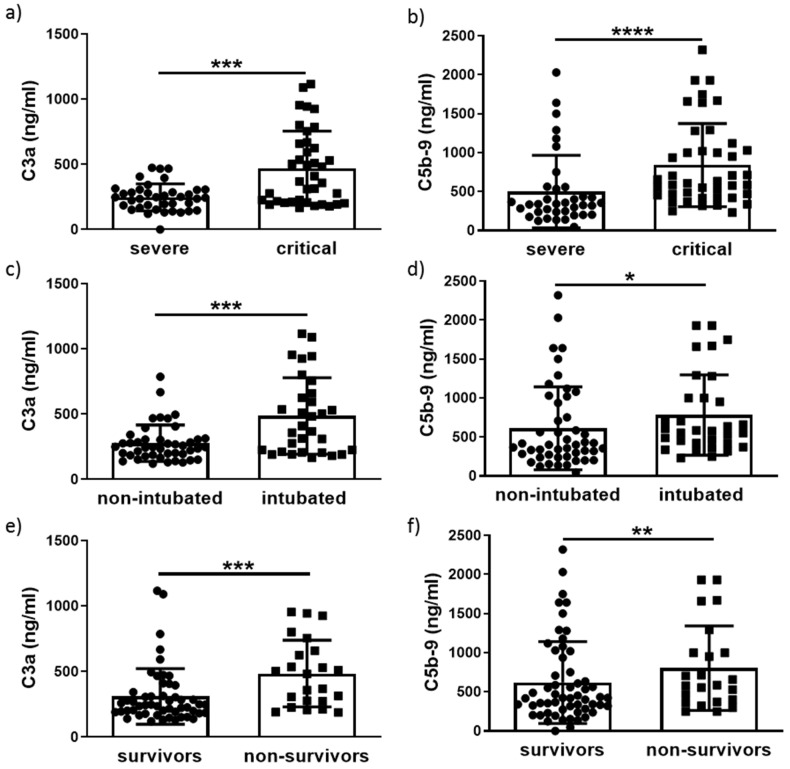
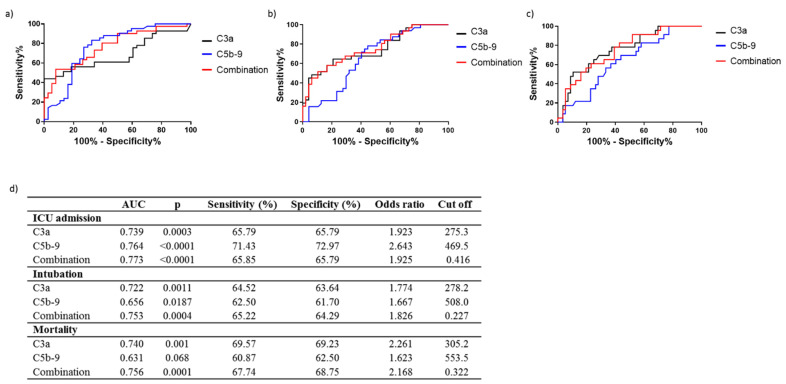
SARS-CoV-2 infection may result in severe pneumonia leading to mechanical ventilation and intensive care (ICU) treatment. Complement activation was verified in COVID-19 and implicated as a contributor to COVID-19 pathogenesis. This study assessed the predictive potential of complement factors C3a and C5b-9 for COVID-19 progression and outcome. We grouped 80 COVID-19 patients into severe COVID-19 patients (n = 38) and critically ill (n = 42) and subdivided into non-intubated (n = 48) and intubated (n = 32), survivors (n = 57) and non-survivors (n = 23). Results: A significant increase for C3a and C5b-9 levels was observed between: severely and critically ill patients (p < 0.001 and p < 0.0001), non-intubated vs intubated (p < 0.001 and p < 0.05), survivors vs non-survivors (p < 0.001 and p < 0.01). ROC analysis for the need for ICU treatment revealed a higher AUC for C5b-9 (0.764, p < 0.001) compared to C3a (AUC = 0.739, p < 0.01). A higher AUC was observed for C3a for the need for intubation (AUC = 0.722, p < 0.001) or mortality (AUC = 0.740, p < 0.0001) compared to C5b-9 (need for intubation AUC = 0.656, p < 0.05 and mortality AUC = 0.631, p = NS). Combining the two markers revealed a powerful prediction tool for ICU admission (AUC = 0.773, p < 0.0001), intubation (AUC = 0.756, p < 0.0001) and mortality (AUC = 0.753, p < 0.001). C3a and C5b-9 may be considered as prognostic tools separately or in combination for the progression and outcome of COVID-19.
Keywords: COVID-19; biomarkers; complement; mortality.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Combination of the CD8+:B-cell and Neutrophil-to-Lymphocyte Ratio as a Novel Prediction Model for Intubation Need and Disease Severity in COVID-19 Patients.In Vivo. 2021 Nov-Dec;35(6):3305-3313. doi: 10.21873/invivo.12626. In Vivo. 2021. PMID: 34697162 Free PMC article.
-
A novel ratio of CD8+:B-cells as a prognostic marker of coronavirus disease 2019 patient progression and outcome.Virology. 2021 Apr;556:79-86. doi: 10.1016/j.virol.2021.01.002. Epub 2021 Jan 13. Virology. 2021. PMID: 33550117 Free PMC article.
-
Lung ultrasound score in establishing the timing of intubation in COVID-19 interstitial pneumonia: A preliminary retrospective observational study.PLoS One. 2020 Sep 3;15(9):e0238679. doi: 10.1371/journal.pone.0238679. eCollection 2020. PLoS One. 2020. Retraction in: PLoS One. 2020 Dec 31;15(12):e0245032. doi: 10.1371/journal.pone.0245032. PMID: 32881950 Free PMC article. Retracted.
-
Prognostic significance of complement factors in severely ill patients with COVID-19.J Investig Med. 2022 Oct;70(7):1466-1471. doi: 10.1136/jim-2021-002224. Epub 2022 Aug 8. J Investig Med. 2022. PMID: 35940732
-
Intensive care for seriously ill patients affected by novel coronavirus sars - CoV - 2: Experience of the Crema Hospital, Italy.Am J Emerg Med. 2021 Jul;45:156-161. doi: 10.1016/j.ajem.2020.08.005. Epub 2020 Aug 16. Am J Emerg Med. 2021. PMID: 33046317 Free PMC article.
Cited by
-
Erythropoietin Effect on Complement Activation in Chronic Kidney Disease.Biomedicines. 2024 Aug 2;12(8):1746. doi: 10.3390/biomedicines12081746. Biomedicines. 2024. PMID: 39200211 Free PMC article.
-
Functional mass spectrometry indicates anti-protease and complement activity increase with COVID-19 severity.Exp Biol Med (Maywood). 2025 Jan 29;250:10308. doi: 10.3389/ebm.2025.10308. eCollection 2025. Exp Biol Med (Maywood). 2025. PMID: 39949890 Free PMC article.
-
Complement and COVID-19: Three years on, what we know, what we don't know, and what we ought to know.Immunobiology. 2023 May;228(3):152393. doi: 10.1016/j.imbio.2023.152393. Epub 2023 May 11. Immunobiology. 2023. PMID: 37187043 Free PMC article. Review.
-
Thrombotic Mechanism Involving Platelet Activation, Hypercoagulability and Hypofibrinolysis in Coronavirus Disease 2019.Int J Mol Sci. 2023 Apr 28;24(9):7975. doi: 10.3390/ijms24097975. Int J Mol Sci. 2023. PMID: 37175680 Free PMC article. Review.
-
CD55 upregulation in T cells of COVID-19 patients suppresses type-I interferon responses.Commun Biol. 2025 May 2;8(1):690. doi: 10.1038/s42003-025-08066-z. Commun Biol. 2025. PMID: 40316776 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
