

High Versus Low Ligation of the Inferior Mesenteric Artery in Colorectal Cancer Surgery: A Systematic Review and Meta-Analysis
- PMID: 36143820
- PMCID: PMC9506533
- DOI: 10.3390/medicina58091143
High Versus Low Ligation of the Inferior Mesenteric Artery in Colorectal Cancer Surgery: A Systematic Review and Meta-Analysis
Abstract
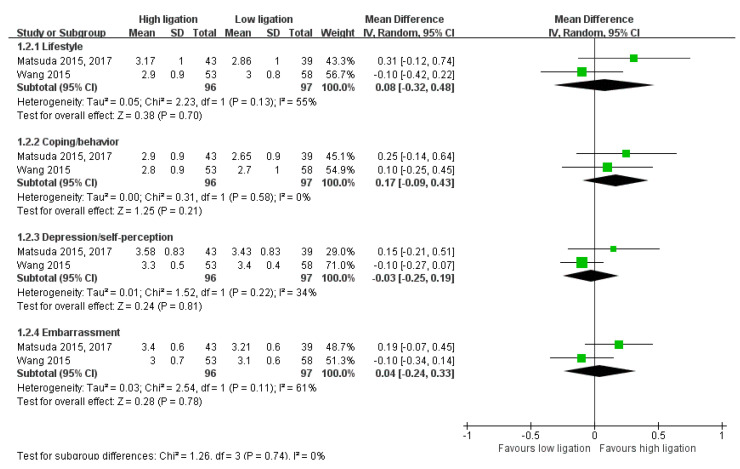
Background and Objectives: This study aimed to compare the effects of high ligation (HL) versus low ligation (LL) in colorectal cancer surgery. Materials and Methods: We performed a comprehensive search using multiple databases (trial registries and ClinicalTrials.gov), other sources of grey literature, and conference proceedings, with no restrictions on the language or publication status, up until 10 March 2021. We included all parallel-group randomized controlled trials (RCTs) and considered cluster RCTs for inclusion. The risk of bias domains were "low risk," "high risk," or "unclear risk." We performed statistical analyses using a random-effects model and interpreted the results according to the Cochrane Handbook for Systematic Reviews of Interventions. We used the GRADE guidelines to rate the certainty of evidence (CoE) of the randomized controlled trials. Results: We found 12 studies (24 articles) from our search. We were very uncertain about the effects of HL on overall mortality, disease recurrence, cancer-specific mortality, postoperative mortality, and anastomotic leakage (very low CoE). There may be little to no difference between HL and LL in postoperative complications (low CoE). For short-term follow-up (within 6 months), HL may reduce defecatory function (constipation; low CoE). While HL and LL may have similar effects on sexual function in men, HL may reduce female sexual function compared with LL (low CoE). For long-term follow-up (beyond 6 months), HL may reduce defecatory function (constipation; low CoE). There were discrepancies in the effects regarding urinary dysfunction according to which questionnaire was used in the studies. HL may reduce male and female sexual function (low CoE). Conclusions: We are very uncertain about the effects of HL on survival outcomes, and there is no difference in the incidence of postoperative complications between HL and LL. More rigorous RCTs are necessary to evaluate the effect of HL and LL on functional outcomes.
Keywords: colorectal cancer; high ligation; inferior mesenteric artery; low ligation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







Similar articles
-
Prostatic arterial embolization for the treatment of lower urinary tract symptoms in men with benign prostatic hyperplasia.Cochrane Database Syst Rev. 2022 Mar 29;3(3):CD012867. doi: 10.1002/14651858.CD012867.pub3. Cochrane Database Syst Rev. 2022. PMID: 35349161 Free PMC article.
-
Taxane monotherapy regimens for the treatment of recurrent epithelial ovarian cancer.Cochrane Database Syst Rev. 2022 Jul 12;7(7):CD008766. doi: 10.1002/14651858.CD008766.pub3. Cochrane Database Syst Rev. 2022. PMID: 35866378 Free PMC article.
-
Acupuncture for treating overactive bladder in adults.Cochrane Database Syst Rev. 2022 Sep 23;9(9):CD013519. doi: 10.1002/14651858.CD013519.pub2. Cochrane Database Syst Rev. 2022. PMID: 36148895 Free PMC article.
-
Oxycodone for cancer-related pain.Cochrane Database Syst Rev. 2022 Jun 9;6(6):CD003870. doi: 10.1002/14651858.CD003870.pub7. Cochrane Database Syst Rev. 2022. PMID: 35679121 Free PMC article.
-
Interventions for great saphenous vein incompetence.Cochrane Database Syst Rev. 2021 Aug 11;8(8):CD005624. doi: 10.1002/14651858.CD005624.pub4. Cochrane Database Syst Rev. 2021. PMID: 34378180 Free PMC article.
Cited by
-
Preserving the left colonic artery in radical sigmoid and rectal cancer surgery is feasible: A meta-analysis.Medicine (Baltimore). 2024 Jan 26;103(4):e37026. doi: 10.1097/MD.0000000000037026. Medicine (Baltimore). 2024. PMID: 38277569 Free PMC article.
-
Inferior mesenteric artery ligation level in rectal cancer surgery: still no answer-a systematic review and meta-analysis.Langenbecks Arch Surg. 2023 Jul 26;408(1):286. doi: 10.1007/s00423-023-03022-z. Langenbecks Arch Surg. 2023. PMID: 37493853 Free PMC article.
References
-
- Kong M., Chen H., Xin Y., Jiang Y., Han Y., Sheng H. High ligation of the inferior mesenteric artery and anastomotic leakage in anterior resection for rectal cancer: A systematic review and meta-analysis of randomized controlled trial studies. Colorectal Dis. 2021;23:614–624. doi: 10.1111/codi.15419. - DOI - PubMed
-
- Alici A., Kement M., Gezen C., Akin T., Vural S., Okkabaz N., Basturk E., Yegenoglu A., Oncel M. Apical lymph nodes at the root of the inferior mesenteric artery in distal colorectal cancer: An analysis of the risk of tumor involvement and the impact of high ligation on anastomotic integrity. Tech. Coloproctol. 2010;14:1–8. doi: 10.1007/s10151-009-0547-6. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
