

α-Tocopherol Pharmacokinetics in Adults with Cystic Fibrosis: Benefits of Supplemental Vitamin C Administration
- PMID: 36145092
- PMCID: PMC9505313
- DOI: 10.3390/nu14183717
α-Tocopherol Pharmacokinetics in Adults with Cystic Fibrosis: Benefits of Supplemental Vitamin C Administration
Abstract
Background: Numerous abnormalities in cystic fibrosis (CF) could influence tocopherol absorption, transportation, storage, metabolism and excretion. We hypothesized that the oxidative distress due to inflammation in CF increases vitamin E utilization, which could be positively influenced by supplemental vitamin C administration.
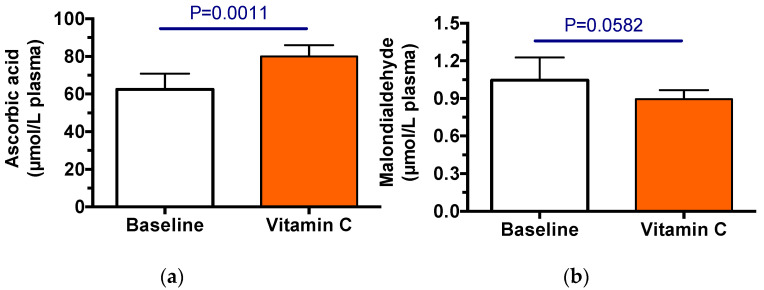
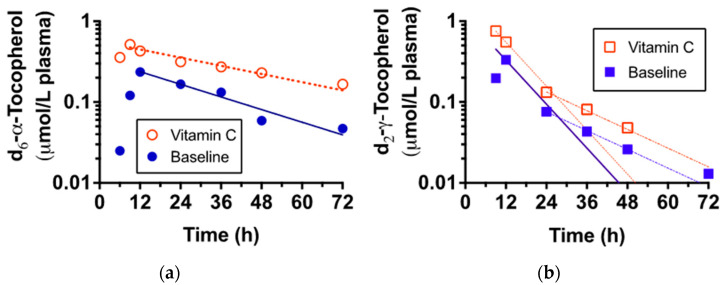
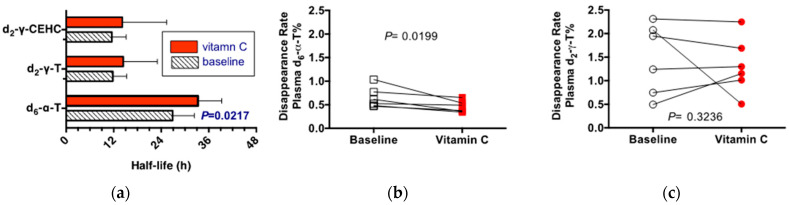
Methods: Immediately before and after receiving vitamin C (500 mg) twice daily for 3.5 weeks, adult CF patients (n = 6) with moderately advanced respiratory tract (RT) disease consumed a standardized breakfast with 30% fat and a capsule containing 50 mg each hexadeuterium (d6)-α- and dideuterium (d2)-γ-tocopheryl acetates. Blood samples were taken frequently up to 72 h; plasma tocopherol pharmacokinetics were determined. During both trials, d6-α- and d2-γ-tocopherols were similarly absorbed and reached similar maximal plasma concentrations ~18-20 h. As predicted, during vitamin C supplementation, the rates of plasma d6-α-tocopherol decline were significantly slower.
Conclusions: The vitamin C-induced decrease in the plasma disappearance rate of α-tocopherol suggests that vitamin C recycled α-tocopherol, thereby augmenting its concentrations. We conclude that some attention should be paid to plasma ascorbic acid concentrations in CF patients, particularly to those individuals with more advanced RT inflammatory disease and including those with severe exacerbations.
Keywords: carboxyethyl hydroxy chromanol (CEHC); stable isotope-labeled vitamin E; vitamin E.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Cystic Fibrosis Foundation 2021 Cystic Fibrosis Foundation Patient Registry Highlights. [(accessed on 16 August 2022)]. Available online: https://www.cff.org/medical-professionals/patient-registry.
-
- Office of Science (OS) Office of Genomics and Precision Public Health. Centers for Diesease Control and Prevention Cystic Fibrosis. [(accessed on 16 August 2022)]; Available online: https://www.cdc.gov/genomics/disease/cystic_fibrosis.htm.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
