

Occurrence of Healthcare-Associated Infections (HAIs) by Escherichia coli and Klebsiella spp. Producing Extended-Spectrum β-lactamases (ESBL) and/or Carbapenemases in Portuguese Long-Term Care Facilities
- PMID: 36145451
- PMCID: PMC9504074
- DOI: 10.3390/pathogens11091019
Occurrence of Healthcare-Associated Infections (HAIs) by Escherichia coli and Klebsiella spp. Producing Extended-Spectrum β-lactamases (ESBL) and/or Carbapenemases in Portuguese Long-Term Care Facilities
Abstract
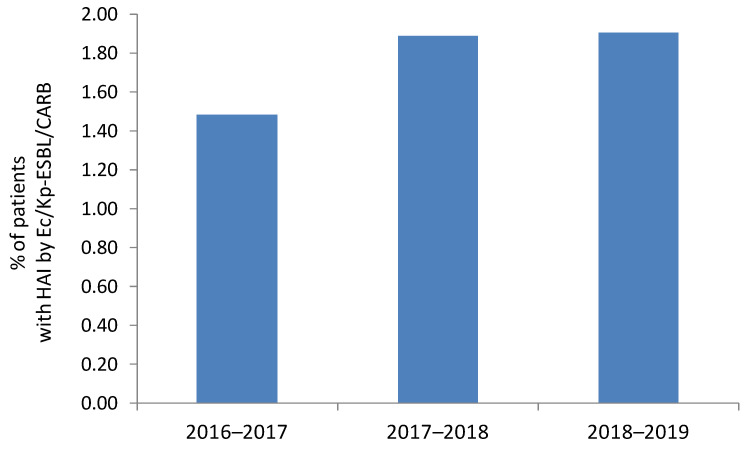
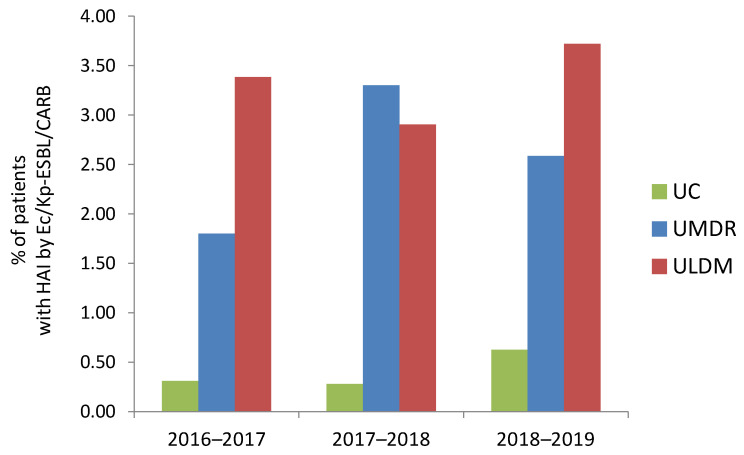
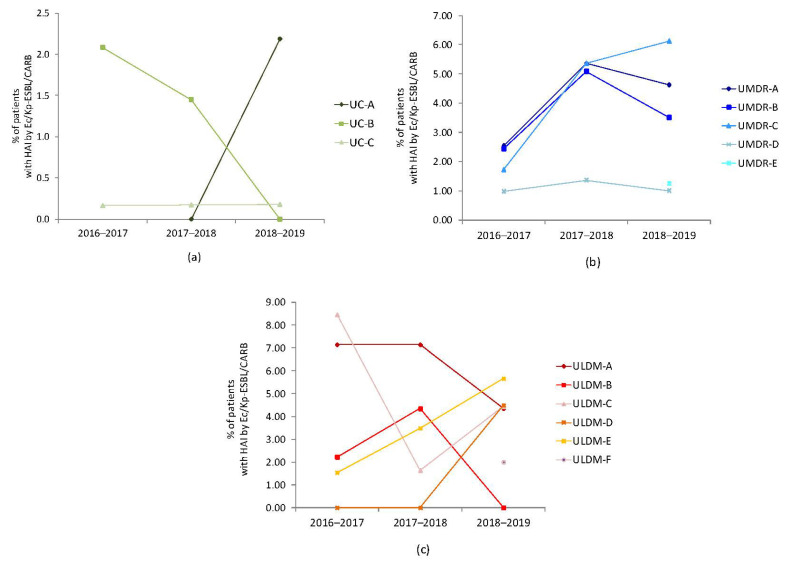
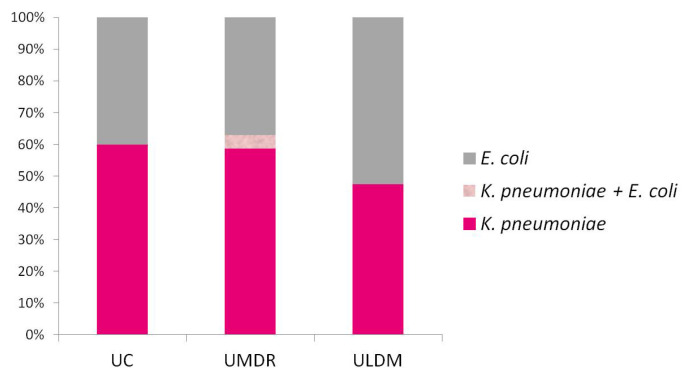
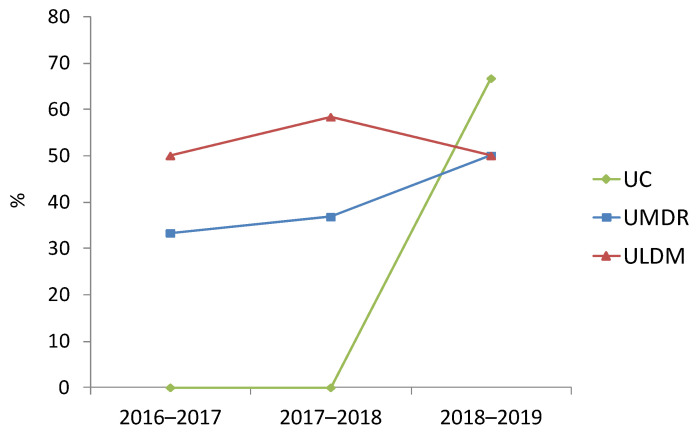
Extended-spectrum-β-lactamase (ESBL)- and carbapenemase-producing bacteria are widespread in hospitals, but the extent of this problem in long-term care facilities (LTCFs) is poorly understood. We aimed to elucidate, in the Portuguese regional clinical context, the relevance of LTCFs as a reservoir of Escherichia coli and Klebsiella spp. producing ESBL- and/or carbapenemases (Ec/Kp-ESBL/CARB). Fourteen LTCFs from Portugal, corresponding to units of convalescence (UC/n = 3), medium-term internment and rehabilitation (UMDR/ n = 5), or long-term internment and maintenance (ULDM/n = 6), were analyzed (2016-2019). All patients with Ec/Kp-ESBL/CARB infections acquired during LTCF stay were included, and detailed information was collected. Prevalence of patients with healthcare-associated infections (HAIs) by Ec/Kp-ESBL/CARB did not vary significantly over time (1.48% in 2016-2017, 1.89% in 2017-2018, and 1.90% in 2018-2019), but a statistically significant association with the LTCF typology (ULDM, UMDR) was observed. HAIs were caused by K. pneumoniae (n = 51/54.3%), E. coli (n = 41/43.6%), or both (n = 2/2.1%), producing ESBL (96%) or carbapenemases (4%). Prior colonization (n = 14/16%) corresponded to seven Kp-CARB and seven Ec/Kp-ESBL. The worrying prevalence of patients acquiring HAIs by Ec/Kp-ESBL/CARB, associated with the estimated rates of those already colonized at admission, highlights a relevant role for LTCFs as a reservoir of Ec/Kp-ESBL/CARB. Epidemiological surveillance should be extended to the national level, and colonization screening at LTCF admission implemented systematically.
Keywords: Enterobacterales; colonization; epidemiological surveillance; extended-spectrum β-lactam antibiotics; resistance.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Infections caused by extended-spectrum β-lactamase-producing Enterobacterales after rectal colonization with ESBL-producing Escherichia coli or Klebsiella pneumoniae.Clin Microbiol Infect. 2020 Aug;26(8):1046-1051. doi: 10.1016/j.cmi.2019.11.025. Epub 2019 Dec 3. Clin Microbiol Infect. 2020. PMID: 31809805
-
Antimicrobial susceptibilities of urinary extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae to fosfomycin and nitrofurantoin in a teaching hospital in Taiwan.J Microbiol Immunol Infect. 2011 Oct;44(5):364-8. doi: 10.1016/j.jmii.2010.08.012. Epub 2011 Jan 20. J Microbiol Immunol Infect. 2011. PMID: 21524974
-
Increasing Incidence of Extended-Spectrum β-Lactamase-Producing Escherichia coli in Community Hospitals throughout the Southeastern United States.Infect Control Hosp Epidemiol. 2016 Jan;37(1):49-54. doi: 10.1017/ice.2015.239. Epub 2015 Oct 13. Infect Control Hosp Epidemiol. 2016. PMID: 26458226 Free PMC article.
-
Review on colonization of residents and staff in Italian long-term care facilities by multidrug-resistant bacteria compared with other European countries.Antimicrob Resist Infect Control. 2016 Oct 11;5:33. doi: 10.1186/s13756-016-0136-1. eCollection 2016. Antimicrob Resist Infect Control. 2016. PMID: 27766146 Free PMC article. Review.
-
The Causes and Control Measures of Extended Spectrum Beta-Lactamase Producing Enterobacteriaceae in Long-Term Care Facilities: A Systematic Review and Meta-Analysis.Health Serv Res Manag Epidemiol. 2022 Oct 17;9:23333928221131709. doi: 10.1177/23333928221131709. eCollection 2022 Jan-Dec. Health Serv Res Manag Epidemiol. 2022. PMID: 36277608 Free PMC article. Review.
Cited by
-
A Novel Bifidobacterium longum Subsp. longum T1 Strain from Cow's Milk: Homeostatic and Antibacterial Activity against ESBL-Producing Escherichia coli.Antibiotics (Basel). 2024 Sep 27;13(10):924. doi: 10.3390/antibiotics13100924. Antibiotics (Basel). 2024. PMID: 39452191 Free PMC article.
-
Prevalence of Carbapenemase and Extended-Spectrum β-Lactamase Producing Enterobacteriaceae: A Cross-Sectional Study.Antibiotics (Basel). 2023 Jan 11;12(1):148. doi: 10.3390/antibiotics12010148. Antibiotics (Basel). 2023. PMID: 36671350 Free PMC article.
References
-
- World Health Organization (WHO) Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report 2021. World Health Organization; Geneva, Switzerland: 2021. [(accessed on 12 June 2022)]. Available online: https://www.who.int/publications/i/item/9789240027336.
-
- World Health Organization (WHO) Regional Office for Europe/European Centre for Disease Prevention and Control (ECDC) Antimicrobial Resistance Surveillance in Europe 2022—2020 Data. WHO Regional Office for Europe; Copenhagen, Denmark: 2022. [(accessed on 12 June 2022)]. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/ECDC-WHO-AMR-re....
LinkOut - more resources
Full Text Sources
Miscellaneous
