

Immunogenic Cell Death Enhances Immunotherapy of Diffuse Intrinsic Pontine Glioma: From Preclinical to Clinical Studies
- PMID: 36145510
- PMCID: PMC9502387
- DOI: 10.3390/pharmaceutics14091762
Immunogenic Cell Death Enhances Immunotherapy of Diffuse Intrinsic Pontine Glioma: From Preclinical to Clinical Studies
Abstract
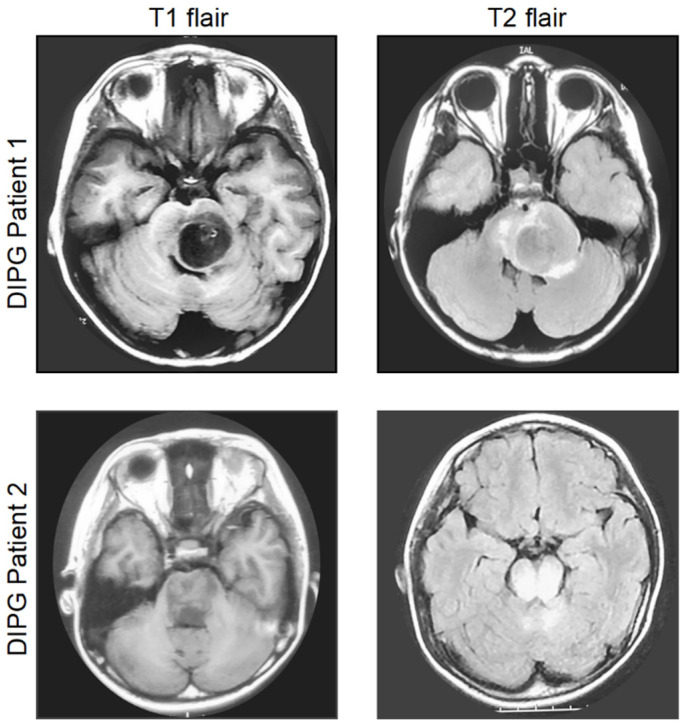
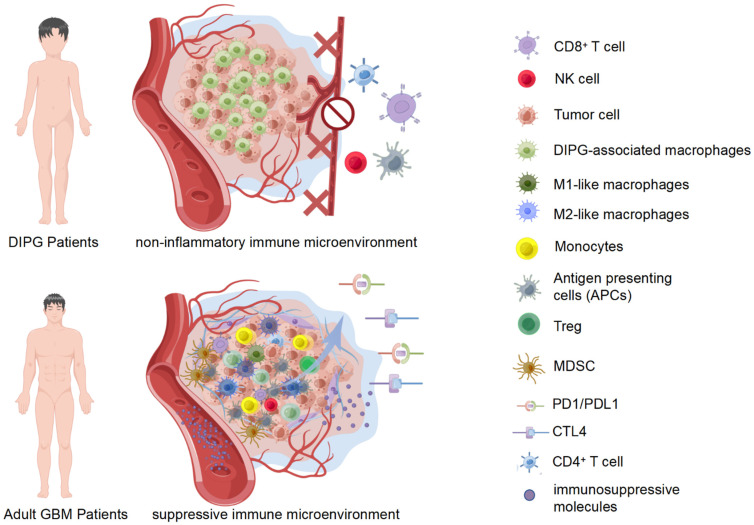
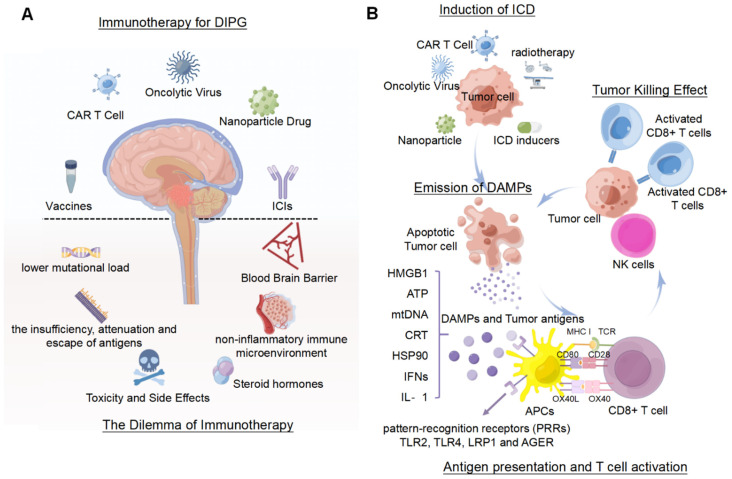
Diffuse intrinsic pontine glioma (DIPG) is the most lethal tumor involving the pediatric central nervous system. The median survival of children that are diagnosed with DIPG is only 9 to 11 months. More than 200 clinical trials have failed to increase the survival outcomes using conventional cytotoxic or myeloablative chemotherapy. Immunotherapy presents exciting therapeutic opportunities against DIPG that is characterized by unique and heterogeneous features. However, the non-inflammatory DIPG microenvironment greatly limits the role of immunotherapy in DIPG. Encouragingly, the induction of immunogenic cell death, accompanied by the release of damage-associated molecular patterns (DAMPs) shows satisfactory efficacy of immune stimulation and antitumor strategies. This review dwells on the dilemma and advances in immunotherapy for DIPG, and the potential efficacy of immunogenic cell death (ICD) in the immunotherapy of DIPG.
Keywords: damage associated molecular patterns; diffuse intrinsic pontine glioma; immune microenvironment; immunogenic cell death; immunotherapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Exploring the tumor microenvironment in diffuse intrinsic pontine glioma: immunological insights and therapeutic challenges.J Immunother Cancer. 2025 Jun 12;13(6):e012009. doi: 10.1136/jitc-2025-012009. J Immunother Cancer. 2025. PMID: 40514066 Free PMC article. Review.
-
Characterization of the immune microenvironment of diffuse intrinsic pontine glioma: implications for development of immunotherapy.Neuro Oncol. 2019 Jan 1;21(1):83-94. doi: 10.1093/neuonc/noy145. Neuro Oncol. 2019. PMID: 30169876 Free PMC article.
-
Non-inflammatory tumor microenvironment of diffuse intrinsic pontine glioma.Acta Neuropathol Commun. 2018 Jun 28;6(1):51. doi: 10.1186/s40478-018-0553-x. Acta Neuropathol Commun. 2018. PMID: 29954445 Free PMC article.
-
Preclinical evaluation of convection-enhanced delivery of liposomal doxorubicin to treat pediatric diffuse intrinsic pontine glioma and thalamic high-grade glioma.J Neurosurg Pediatr. 2017 May;19(5):518-530. doi: 10.3171/2016.9.PEDS16152. Epub 2017 Feb 17. J Neurosurg Pediatr. 2017. PMID: 28291423
-
Immune Microenvironment and Immunotherapies for Diffuse Intrinsic Pontine Glioma.Cancers (Basel). 2023 Jan 18;15(3):602. doi: 10.3390/cancers15030602. Cancers (Basel). 2023. PMID: 36765560 Free PMC article. Review.
Cited by
-
Epidemiology, Diagnostic Strategies, and Therapeutic Advances in Diffuse Midline Glioma.J Clin Med. 2023 Aug 12;12(16):5261. doi: 10.3390/jcm12165261. J Clin Med. 2023. PMID: 37629304 Free PMC article. Review.
-
Opportunities and challenges related to ferroptosis in glioma and neuroblastoma.Front Oncol. 2023 Mar 2;13:1065994. doi: 10.3389/fonc.2023.1065994. eCollection 2023. Front Oncol. 2023. PMID: 36937406 Free PMC article. Review.
-
Exploring the tumor microenvironment in diffuse intrinsic pontine glioma: immunological insights and therapeutic challenges.J Immunother Cancer. 2025 Jun 12;13(6):e012009. doi: 10.1136/jitc-2025-012009. J Immunother Cancer. 2025. PMID: 40514066 Free PMC article. Review.
-
Ghost messages: cell death signals spread.Cell Commun Signal. 2023 Jan 9;21(1):6. doi: 10.1186/s12964-022-01004-0. Cell Commun Signal. 2023. PMID: 36624476 Free PMC article. Review.
References
-
- Gupta N., Goumnerova L.C., Manley P., Chi S.N., Neuberg D., Puligandla M., Fangusaro J., Goldman S., Tomita T., Alden T., et al. Prospective feasibility and safety assessment of surgical biopsy for patients with newly diagnosed diffuse intrinsic pontine glioma. Neuro-Oncology. 2018;20:1547–1555. doi: 10.1093/neuonc/noy070. - DOI - PMC - PubMed
-
- Cooney T., Lane A., Bartels U., Bouffet E., Goldman S., Leary S.E.S., Foreman N.K., Packer R.J., Broniscer A., Minturn J.E., et al. Contemporary survival endpoints: An International Diffuse Intrinsic Pontine Glioma Registry study. Neuro-Oncol. 2017;19:1279–1280. doi: 10.1093/neuonc/nox107. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
