

The Impact of Low Cardiac Output on Propofol Pharmacokinetics across Age Groups-An Investigation Using Physiologically Based Pharmacokinetic Modelling
- PMID: 36145705
- PMCID: PMC9502676
- DOI: 10.3390/pharmaceutics14091957
The Impact of Low Cardiac Output on Propofol Pharmacokinetics across Age Groups-An Investigation Using Physiologically Based Pharmacokinetic Modelling
Abstract
Background: pathophysiological changes such as low cardiac output (LCO) impact pharmacokinetics, but its extent may be different throughout pediatrics compared to adults. Physiologically based pharmacokinetic (PBPK) modelling enables further exploration.
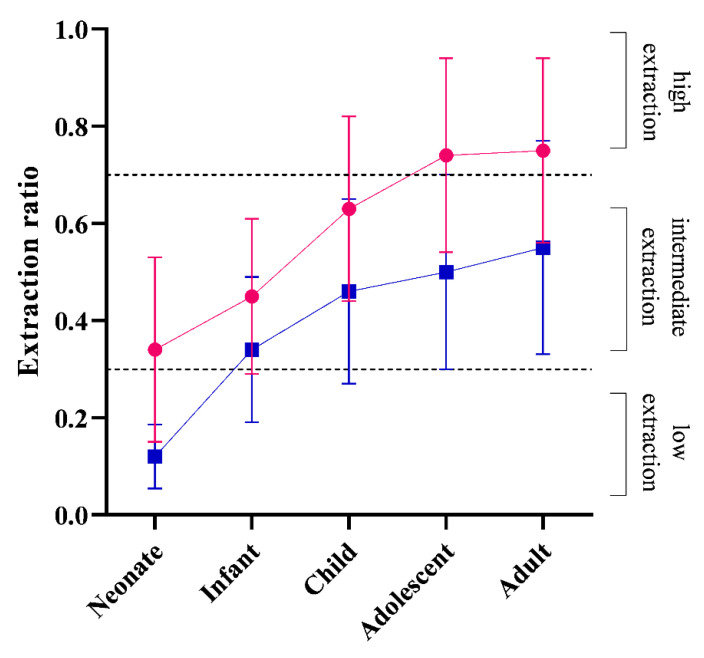
Methods: A validated propofol model was used to simulate the impact of LCO on propofol clearance across age groups using the PBPK platform, Simcyp® (version 19). The hepatic and renal extraction ratio of propofol was then determined in all age groups. Subsequently, manual infusion dose explorations were conducted under LCO conditions, targeting a 3 µg/mL (80-125%) propofol concentration range.
Results: Both hepatic and renal extraction ratios increased from neonates, infants, children to adolescents and adults. The relative change in clearance following CO reductions increased with age, with the least impact of LCO in neonates. The predicted concentration remained within the 3 µg/mL (80-125%) range under normal CO and LCO (up to 30%) conditions in all age groups. When CO was reduced by 40-50%, a dose reduction of 15% is warranted in neonates, infants and children, and 25% in adolescents and adults.
Conclusions: PBPK-driven, the impact of reduced CO on propofol clearance is predicted to be age-dependent, and proportionally greater in adults. Consequently, age group-specific dose reductions for propofol are required in LCO conditions.
Keywords: asphyxia; developmental pharmacology; hypothermia; low cardiac output; neonate; pediatrics; pharmacokinetics; physiologically based pharmacokinetic modelling; propofol.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



Similar articles
-
The use of PBPK modeling across the pediatric age range using propofol as a case.J Pharmacokinet Pharmacodyn. 2018 Dec;45(6):765-785. doi: 10.1007/s10928-018-9607-8. Epub 2018 Oct 8. J Pharmacokinet Pharmacodyn. 2018. PMID: 30298439
-
Physiologically based pharmacokinetic modelling of acetaminophen in preterm neonates-The impact of metabolising enzyme ontogeny and reduced cardiac output.Biopharm Drug Dispos. 2021 Nov;42(9):401-417. doi: 10.1002/bdd.2301. Epub 2021 Aug 28. Biopharm Drug Dispos. 2021. PMID: 34407204
-
The effect of cardiac output on the pharmacokinetics and pharmacodynamics of propofol during closed-loop induction of anesthesia.Comput Methods Programs Biomed. 2020 Aug;192:105406. doi: 10.1016/j.cmpb.2020.105406. Epub 2020 Feb 19. Comput Methods Programs Biomed. 2020. PMID: 32155533
-
A manual propofol infusion regimen for neonates and infants.Paediatr Anaesth. 2019 Sep;29(9):907-914. doi: 10.1111/pan.13706. Epub 2019 Aug 12. Paediatr Anaesth. 2019. PMID: 31325395
-
Propofol context-sensitive decrement times in children.Paediatr Anaesth. 2022 Mar;32(3):396-403. doi: 10.1111/pan.14391. Epub 2022 Jan 10. Paediatr Anaesth. 2022. PMID: 34971456 Review.
Cited by
-
Personalized Dosing of Medicines for Children: A Primer on Pediatric Pharmacometrics for Clinicians.Paediatr Drugs. 2024 Jul;26(4):365-379. doi: 10.1007/s40272-024-00633-x. Epub 2024 May 16. Paediatr Drugs. 2024. PMID: 38755515 Free PMC article. Review.
-
Physiologically Based Pharmacokinetic Modeling in Neonates: Current Status and Future Perspectives.Pharmaceutics. 2023 Dec 12;15(12):2765. doi: 10.3390/pharmaceutics15122765. Pharmaceutics. 2023. PMID: 38140105 Free PMC article. Review.
-
Advances in Canine Anesthesia: Physiologically Based Pharmacokinetic Modeling for Predicting Propofol Plasma Profiles in Canines with Hepatic Impairment.Pharmaceuticals (Basel). 2024 Dec 19;17(12):1720. doi: 10.3390/ph17121720. Pharmaceuticals (Basel). 2024. PMID: 39770561 Free PMC article.
References
-
- Leslie K., Sessler D.I., Bjorksten A.R., Moayeri A. Mild hypothermia alters propofol pharmacokinetics and increases the duration of action of atracurium. Anesth. Analg. 1995;80:1007–1014. - PubMed
LinkOut - more resources
Full Text Sources
