

Recent Advances in Glioma Cancer Treatment: Conventional and Epigenetic Realms
- PMID: 36146527
- PMCID: PMC9501259
- DOI: 10.3390/vaccines10091448
Recent Advances in Glioma Cancer Treatment: Conventional and Epigenetic Realms
Abstract
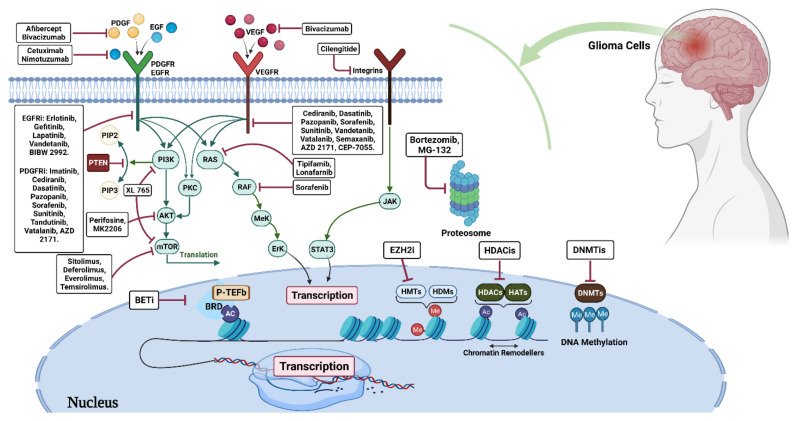
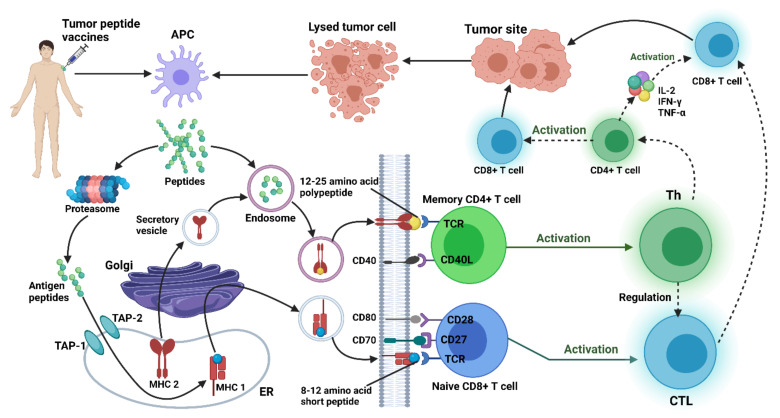
Glioblastoma (GBM) is the most typical and aggressive form of primary brain tumor in adults, with a poor prognosis. Successful glioma treatment is hampered by ineffective medication distribution across the blood-brain barrier (BBB) and the emergence of drug resistance. Although a few FDA-approved multimodal treatments are available for glioblastoma, most patients still have poor prognoses. Targeting epigenetic variables, immunotherapy, gene therapy, and different vaccine- and peptide-based treatments are some innovative approaches to improve anti-glioma treatment efficacy. Following the identification of lymphatics in the central nervous system, immunotherapy offers a potential method with the potency to permeate the blood-brain barrier. This review will discuss the rationale, tactics, benefits, and drawbacks of current glioma therapy options in clinical and preclinical investigations.
Keywords: brain tumor; cancer; epigenetic; glioblastoma; peptide-based treatment; treatment; vaccine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Overcoming the blood-brain tumor barrier for effective glioblastoma treatment.Drug Resist Updat. 2015 Mar;19:1-12. doi: 10.1016/j.drup.2015.02.002. Epub 2015 Mar 6. Drug Resist Updat. 2015. PMID: 25791797 Review.
-
Combinatorial approaches to effective therapy in glioblastoma (GBM): Current status and what the future holds.Int Rev Immunol. 2022;41(6):582-605. doi: 10.1080/08830185.2022.2101647. Epub 2022 Aug 8. Int Rev Immunol. 2022. PMID: 35938932 Review.
-
Enhancement of Therapies for Glioblastoma (GBM) Using Nanoparticle-based Delivery Systems.AAPS PharmSciTech. 2021 Feb 11;22(2):71. doi: 10.1208/s12249-021-01928-9. AAPS PharmSciTech. 2021. PMID: 33575970 Free PMC article. Review.
-
Current Approaches for Glioma Gene Therapy and Virotherapy.Front Mol Neurosci. 2021 Mar 11;14:621831. doi: 10.3389/fnmol.2021.621831. eCollection 2021. Front Mol Neurosci. 2021. PMID: 33790740 Free PMC article. Review.
-
Multimodal targeting of glioma with functionalized nanoparticles.Cancer Cell Int. 2022 Aug 23;22(1):265. doi: 10.1186/s12935-022-02687-8. Cancer Cell Int. 2022. PMID: 35999629 Free PMC article. Review.
Cited by
-
Mucins as Precision Biomarkers in Glioma: Emerging Evidence for Their Potential in Biospecimen Analysis and Outcome Prediction.Biomedicines. 2024 Dec 11;12(12):2806. doi: 10.3390/biomedicines12122806. Biomedicines. 2024. PMID: 39767713 Free PMC article. Review.
-
Clusterin-mediated polarization of M2 macrophages: a mechanism of temozolomide resistance in glioblastoma stem cells.Stem Cell Res Ther. 2025 Mar 24;16(1):146. doi: 10.1186/s13287-025-04247-z. Stem Cell Res Ther. 2025. PMID: 40128761 Free PMC article.
-
Dual roles of extracellular vesicles in acute lymphoblastic leukemia: implications for disease progression and theranostic strategies.Med Oncol. 2024 Nov 22;42(1):11. doi: 10.1007/s12032-024-02547-7. Med Oncol. 2024. PMID: 39572459 Free PMC article. Review.
-
Reprogramming of astrocytes to neuronal-like cells in spinal cord injury: a systematic review.Spinal Cord. 2024 Apr;62(4):133-142. doi: 10.1038/s41393-024-00969-8. Epub 2024 Mar 6. Spinal Cord. 2024. PMID: 38448665
-
Advancements in dendritic cell vaccination: enhancing efficacy and optimizing combinatorial strategies for the treatment of glioblastoma.Front Neurol. 2023 Oct 31;14:1271822. doi: 10.3389/fneur.2023.1271822. eCollection 2023. Front Neurol. 2023. PMID: 38020665 Free PMC article. Review.
References
-
- Nicholson J.G., Fine H.A. Diffuse Glioma Heterogeneity and Its Therapeutic Implications. Cancer Discov. 2021;11:575–590. doi: 10.1158/2159-8290.CD-20-1474. - DOI - PubMed
-
- Park J., Shim J.-K., Kang J.H., Choi J., Chang J.H., Kim S.-Y., Kang S.-G. Regulation of bioenergetics through dual inhibition of aldehyde dehydrogenase and mitochondrial complex I suppresses glioblastoma tumorspheres. Neuro-Oncology. 2018;20:954–965. doi: 10.1093/neuonc/nox243. - DOI - PMC - PubMed
-
- Geng F., Cheng X., Wu X., Yoo J.Y., Cheng C., Guo J.Y., Mo X., Ru P., Hurwitz B., Kim S.-H. Inhibition of SOAT1 Suppresses Glioblastoma Growth via Blocking SREBP-1–Mediated LipogenesisTargeting SOAT1 to Treat Glioblastoma. Clin. Cancer Res. 2016;22:5337–5348. doi: 10.1158/1078-0432.CCR-15-2973. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
