

Diagnostic performance of exercise stress tests for detection of epicardial and microvascular coronary artery disease: the UZ Clear study
- PMID: 36147027
- PMCID: PMC9909457
- DOI: 10.4244/EIJ-D-22-00270
Diagnostic performance of exercise stress tests for detection of epicardial and microvascular coronary artery disease: the UZ Clear study
Abstract
Background: Cardiac stress tests remain the cornerstone for evaluating patients suspected of having obstructive coronary artery disease (CAD). Coronary microvascular dysfunction (CMD) can lead to abnormal non-invasive tests.
Aims: We sought to assess the diagnostic performance of exercise stress tests with indexes of epicardial and microvascular resistance as reference.
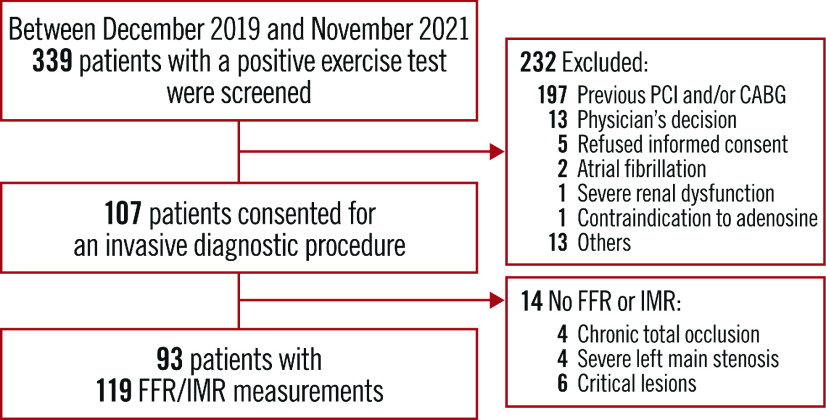
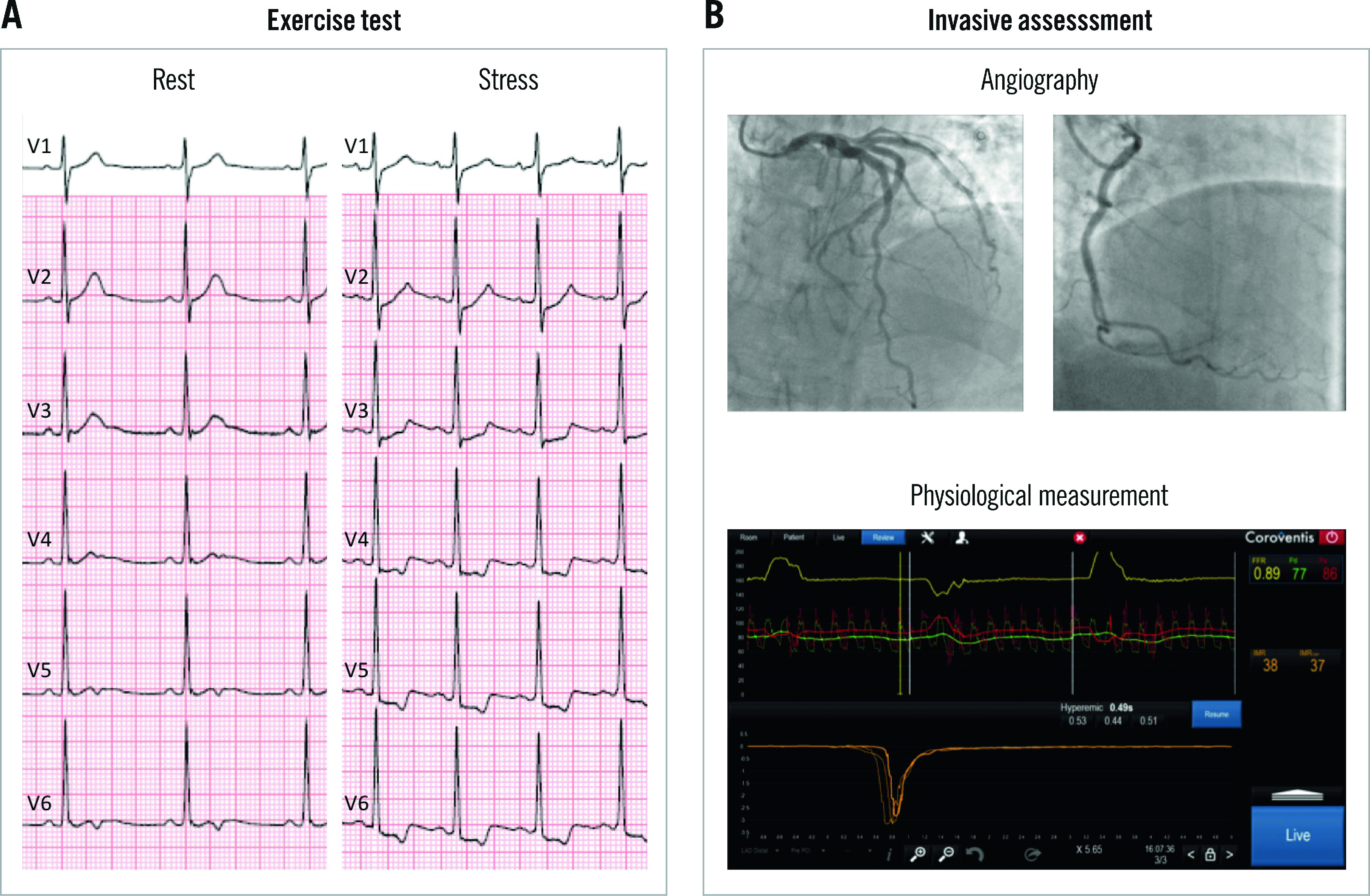
Methods: This was a prospective, single-arm, multicentre study of patients with an intermediate pretest probability of CAD and positive exercise stress tests who were referred for invasive angiography. Patients underwent an invasive diagnostic procedure (IDP) with measurement of fractional flow reserve (FFR) and index of microvascular resistance (IMR) in at least one coronary vessel. Obstructive CAD was defined as diameter stenosis (DS) >50% by quantitative coronary angiography (QCA). The objective was to determine the false discovery rate (FDR) of cardiac exercise stress tests with both FFR and IMR as references.
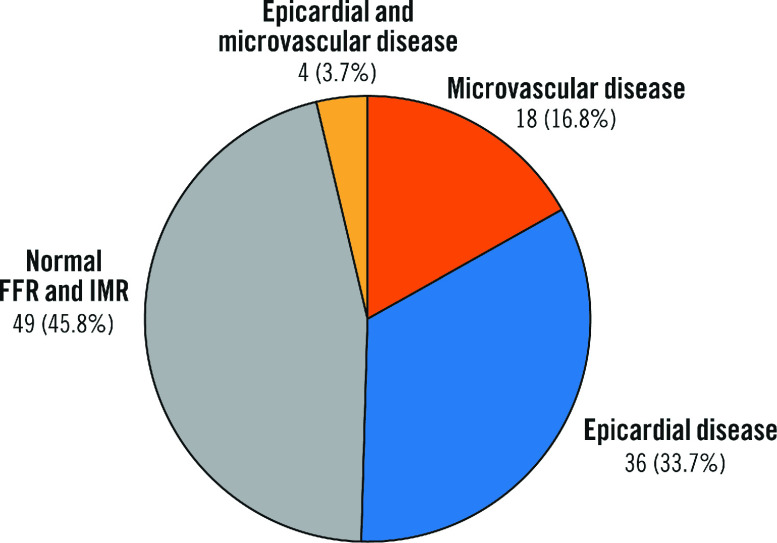
Results: One hundred and seven patients (137 vessels) were studied. The mean age was 62.1±8.7, and 27.1% were female. The mean diameter stenosis was 37.2±27.5%, FFR was 0.84±0.10, coronary flow reserve was 2.74±2.07, and IMR 20.3±11.9. Obstructive CAD was present in 39.3%, whereas CMD was detected in 20.6%. The FDR was 60.7% and 62.6% with QCA and FFR as references (p-value=0.803). The combination of FFR and IMR as clinical reference reduced the FDR by 25% compared to QCA (45.8% vs 60.7%; p-value=0.006).
Conclusions: In patients with evidence of ischaemia, an invasive functional assessment accounting for the epicardial and microvascular compartments led to an improvement in the diagnostic performance of exercise tests, driven by a significant FDR reduction.
Conflict of interest statement
D. Andreini reports receiving research grants from GE Healthcare and Bracco. T. Mizukami reports receiving consulting fees from Zeon Medical, research grants from Boston Scientific, and speaker fees from Abbott, CathWorks, and Boston Scientific. N. Mileva reports receiving speaker fees from Abbott. D. Munhoz reports receiving research grants provided by the CardioPaTh PhD program. E. Barbato reports receiving speaker's fees from Boston Scientific, Abbott, GE Healthcare, Insight Lifetech, and OpSens. B. De Bruyne reports receiving consultancy fees from Boston Scientific and Abbott, research grants from Coroventis Research, Pie Medical Imaging, CathWorks, Boston Scientific, Siemens, HeartFlow, and Abbott, and owning equity in Siemens, GE Healthcare, Philips, HeartFlow, Edwards Lifesciences, Bayer, Sanofi, and Celyad. B. Cosyns reports receiving consulting fees from Philips and Boehringer Ingelheim, participation on the Board of Novartis and Pfizer; is President of the EACVI; and is a board member of the ESC and the Belgian Society of Cardiology. C. Collet reports receiving research grants from Biosensors International, Coroventis Research, Medis Medical Imaging, Pie Medical Imaging, CathWorks, Boston Scientific, Siemens, HeartFlow, and Abbott, and consultancy fees from HeartFlow, OpSens, Abbott, and Philips. The other authors have no conflicts of interest to declare.
Figures


References
-
- Writing Committee, Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, Blankstein R, Boyd J, Bullock-Palmer RP, Conejo T, Diercks DB, Gentile F, Greenwood JP, Hess EP, Hollenberg SM, Jaber WA, Jneid H, Joglar JA, Morrow DA, O'Connor RE, Ross MA, Shaw LJ. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021;78:2218–61. - PubMed
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407–77. - PubMed
-
- Gianrossi R, Detrano R, Mulvihill D, Lehmann K, Dubach P, Colombo A, McArthur D, Froelicher V. Exercise-induced ST depression in the diagnosis of coronary artery disease. A meta-analysis. Circulation. 1989;80:87–98. - PubMed
-
- De Bruyne, Hersbach F, Pijls NH, Bartunek J, Bech JW, Heyndrickx GR, Gould KL, Wijns W. Abnormal epicardial coronary resistance in patients with diffuse atherosclerosis but ‘Normal’ coronary angiography. Circulation. 2001;104:2401–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous