

Case Reports
doi: 10.1016/j.jdcr.2022.03.026.
eCollection 2022 Oct.
IgG/IgA pemphigus with differing regional presentations
Affiliations
- PMID: 36147207
- PMCID: PMC9486352
- DOI: 10.1016/j.jdcr.2022.03.026
Item in Clipboard
Case Reports
IgG/IgA pemphigus with differing regional presentations
JAAD Case Rep.
.
No abstract available
Keywords: DIF, direct immunofluorescence; ELISA; ELISA, enzyme-linked immunosorbent assay; Ig, immunoglobulin; IgA; IgG; desmoglein; direct immunofluorescence; intercellular; pemphigus; scalp.
Conflict of interest statement
None disclosed.
Figures
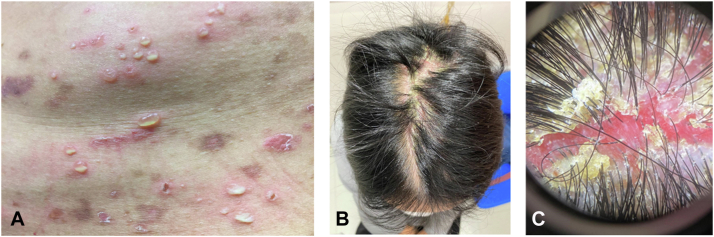
A, The truncal blisters taken at the upper abdomen. The blisters were large and tense, scattered throughout the truncal region and involved the proximal parts of the four limbs. Peri-blister erythema was evident. Hypopyon formation was seen in some of the blisters. Some of the blisters had already resolved, leaving behind post-inflammatory hyper-pigmentation. Scarring was not seen. B, There were scaling and erythema localized over the scalp midline, extending antero-posteriorly. Despite an extensive involvement, there was no scarring alopecia or appreciable hair shedding. The scalp condition was entirely asymptomatic. C, A dermoscopic view of the thick scale that entangled the base of the hair shafts. The underlying scalp surface was erythematous, friable and moist. Abnormal vascular pattern, surface erosion and ulceration were not found. There was no evidence of tinea capitis.
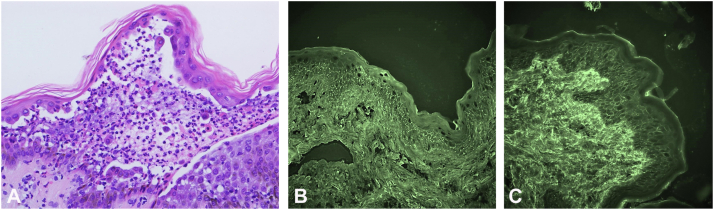
A, Truncal blister skin biopsy, featuring intra-epidermal acantholysis, dense neutrophilic and occasional eosinophilic infiltrates. There was no interface dermatitis, pigmentary incontinence, viral cytopathic effect or fungal hyphae. (H&E stain, 400×). B, The second skin biopsy for direct immunofluorescence, IgA with fluorescein isothiocyanate. Note the intercellular net-like positivity over the lower one- to two-thirds of the epidermis. Non-specific background staining was noted in the dermal collagen bundles. (Direct immunofluorescence microscopy, ×100). C, The second skin biopsy for direct immunofluorescence, IgG with fluorescein isothiocyanate. Note the intercellular net-like positivity throughout the entire epidermis. Non-specific background staining was noted in the dermal collagen. (Direct immunofluorescence microscopy, ×100).

A, Medium power view of the scalp biopsy. Note the extensive intra-epidermal and intra-follicular splitting secondary to the acantholysis. There was no interface dermatitis, thickening of basement membrane or keratinocytic viral cytopathic effect. The papillary dermis was oedematous and capillaries markedly engorged. The inflammatory infiltrates comprised mainly of neutrophils, rarely eosinophils and lymphocytes. (H&E stain, 100×). B, Scalp punch biopsy for direct immunofluorescence, IgA with fluorescein isothiocyanate. Note the intercellular net-like positivity over the epidermis. There was a non-specific background staining within the dermal collagen bundles. (Direct immunofluorescence microscopy, ×40). C, Scalp punch biopsy for direct immunofluorescence, IgG with fluorescein isothiocyanate. Note the intercellular net-like positivity over the entire epidermis. There was a non-specific background staining within the dermal collagen bundles. (Direct immunofluorescence microscopy, ×40).
References
-
- Wallach D., Foldès C., Cottenot F. Pustulose sous-cornée, acantholyse superficielle et IgA monoclonale. Ann Dermatol Venereol. 2000;127(11):1037–1041. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous