

Phenotypic prevalence of obesity and metabolic syndrome among an underdiagnosed and underscreened population of over 50 million children and adults
- PMID: 36147487
- PMCID: PMC9485995
- DOI: 10.3389/fgene.2022.961116
Phenotypic prevalence of obesity and metabolic syndrome among an underdiagnosed and underscreened population of over 50 million children and adults
Abstract
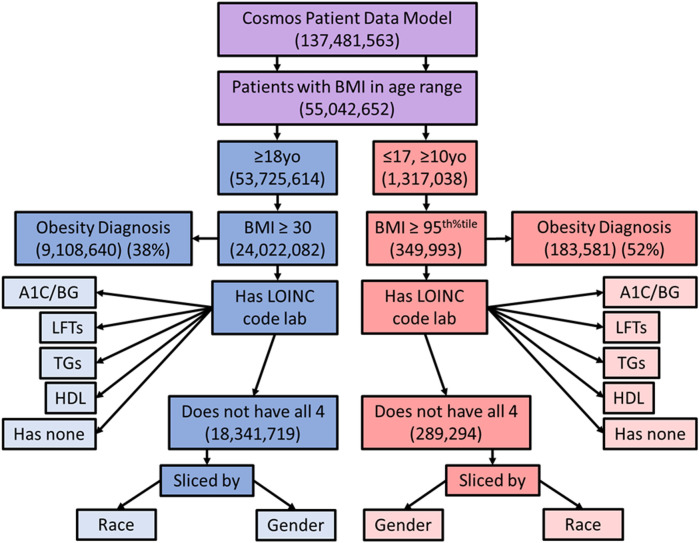
Background: Metabolic syndrome is a phenotypic condition associated with a variety of genotypes. Studies of rare genotypes can be made more difficult by clinical underscreening of the population for the phenotypic traits that define metabolic syndrome to clinicians. Studies have demonstrated underdiagnosis of pediatric obesity, as well as reduced rates of pediatric screening for obesity related conditions, including conditions leading to a diagnosis of metabolic syndrome. If true, there may be a significant underdiagnosis of metabolic syndrome among the pediatric population compared to the adult population. Methods: Using Epic's Cosmos Data Network aggregated, de-identified patient data collected from healthcare organizations using the Epic electronic health record (EHR), we examined obesity and metabolic syndrome rates among adult and pediatric patients. We also examined screening rates for obesity related conditions and metabolic syndrome among adult and pediatric patients across the United States. We also sought to compare rates between subgroups within the population including age, sex, and race. Results: In our population, 45% of adults and 27% of pediatric population were obese by age and gender specific BMI criteria. 38% of the obese adult population had an ICD-10 code associated with the diagnosis vs. 52% of the pediatric population. Of adults meeting obesity criteria, 36% had results for appropriate, guideline-based blood laboratory testing for insulin resistance, 40-42% for dyslipidemia, and 55% for hepatic steatosis. 36% of obese adult patients had none of the recommended blood laboratory testing. 31% of the adult population met diagnostic criteria for metabolic syndrome. Of pediatric patients meeting obesity criteria, 27% had results for appropriate blood laboratory testing for insulin resistance, 28% for dyslipidemia, and 33% for hepatic steatosis. 59% of obese pediatric patients had none of the recommended blood laboratory testing. 3% of the pediatric population met criteria for diagnosis of metabolic syndrome. Discussion: This study represents one of the largest multicenter national cohorts assembled for studying metabolic syndrome (over 50 million patients) and demonstrates the power of emerging aggregated EHR tools for research. Although obesity is better diagnosed in pediatric patients than in adult patients, significantly lower screening rates for obesity related conditions occurred in pediatric patients compared to adults. Statistically significant, but clinically negligible differences in screening rates were found by race and gender. These results support smaller prior studies that suggest that obesity is under-diagnosed and obesity related conditions underscreened in pediatric and adult populations, and additionally suggests underdiagnosis of metabolic syndrome among United States pediatric and adult patients.
Keywords: adolescents; cosmos; epic; metabolic syndrome; obesity; pediatric.
Copyright © 2022 Kim and Kaelber.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous