

Clinical Implementation of Combined Monogenic and Polygenic Risk Disclosure for Coronary Artery Disease
- PMID: 36147540
- PMCID: PMC9491373
- DOI: 10.1016/j.jacadv.2022.100068
Clinical Implementation of Combined Monogenic and Polygenic Risk Disclosure for Coronary Artery Disease
Abstract
Background: State-of-the-art genetic risk interpretation for a common complex disease such as coronary artery disease (CAD) requires assessment for both monogenic variants-such as those related to familial hypercholesterolemia-as well as the cumulative impact of many common variants, as quantified by a polygenic score.
Objectives: The objective of the study was to describe a combined monogenic and polygenic CAD risk assessment program and examine its impact on patient understanding and changes to clinical management.
Methods: Study participants attended an initial visit in a preventive genomics clinic and a disclosure visit to discuss results and recommendations, primarily via telemedicine. Digital postdisclosure surveys and chart review evaluated the impact of disclosure.
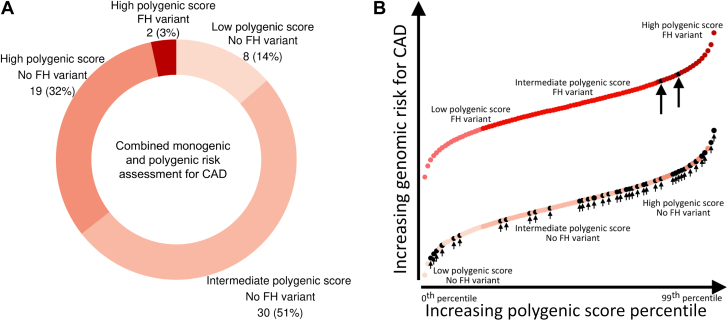
Results: There were 60 participants (mean age 51 years, 37% women, 72% with no known CAD), including 30 (50%) referred by their cardiologists and 30 (50%) self-referred. Two (3%) participants had a monogenic variant pathogenic for familial hypercholesterolemia, and 19 (32%) had a high polygenic score in the top quintile of the population distribution. In a postdisclosure survey, both the genetic test report (in 80% of participants) and the discussion with the clinician (in 89% of participants) were ranked as very or extremely helpful in understanding the result. Of the 42 participants without CAD, 17 or 40% had a change in management, including statin initiation, statin intensification, or coronary imaging.
Conclusions: Combined monogenic and polygenic assessments for CAD risk provided by preventive genomics clinics are beneficial for patients and result in changes in management in a significant portion of patients.
Keywords: coronary artery disease; genetics; genomic medicine; polygenic score; precision medicine; preventive cardiology.
Conflict of interest statement
Funding support was provided by grants 1K08HG010155 and 1U01HG011719 (to Dr Khera) from the National Human Genome Research Institute, a Hassenfeld Scholar Award from Massachusetts General Hospital (to Dr Khera), a Merkin Institute Fellowship, and institutional SPARC award from the Broad Institute of MIT and Harvard (to Dr Khera), and a sponsored research agreement from IBM Research (to Dr Khera). Dr Ng is an employee of IBM Research. Drs Zhou and Neben and Mr Okumura are employed by and may have an equity interest in Color Health. Dr Philippakis has received research support from Bayer AG, IBM, Intel, and Verily; and has consulted for Novartis and Rakuten. Dr Natarajan has received grant support from Amgen, Apple, AstraZeneca, Novartis, and Boston Scientific; consulting income from Apple, AstraZeneca, Genentech/Roche, Blackstone Life Sciences, Foresite Labs, Novartis, and TenSixteen Bio; is a member of the scientific advisory board and shareholder of TenSixteen Bio and geneXwell; and spousal employment and equity in Vertex, all unrelated to the present work. Dr Ellinor has received sponsored research support from Bayer AG and IBM Research; and has consulted for Bayer AG, Novartis, and MyoKardia. Dr Khera is an employee and holds equity in Verve Therapeutics; has served as a scientific advisor to Amgen, Maze Therapeutics, Navitor Pharmaceuticals, Sarepta Therapeutics, Novartis, Silence Therapeutics, Korro Bio, Veritas International, Color Health, Third Rock Ventures, Foresite Labs, and Columbia University (National Institute of Health); received speaking fees from Illumina, MedGenome, Amgen, and the Novartis Institute for Biomedical Research; and received a sponsored research agreement from IBM Research. Dr Fahed is a consultant and owns shares in Goodpath. All other authors have reported that they have no relationships relevant to the contents of this paper.
Figures



Comment in
-
The Road Toward Clinical Implementation of Polygenic Risk Scores for Coronary Artery Disease.JACC Adv. 2022 Aug 26;1(3):100071. doi: 10.1016/j.jacadv.2022.100071. eCollection 2022 Aug. JACC Adv. 2022. PMID: 38938397 Free PMC article.
References
-
- Arnett D.K., Blumenthal R.S., Albert M.A., et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;74(10):e177–e232. - PMC - PubMed
-
- Grundy S.M., Stone N.J., Bailey A.L., et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73(24):3168–3209. doi: 10.1016/j.jacc.2018.11.002. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
