

Time trends in tuberculosis mortality across the BRICS: an age-period-cohort analysis for the GBD 2019
- PMID: 36147625
- PMCID: PMC9486016
- DOI: 10.1016/j.eclinm.2022.101646
Time trends in tuberculosis mortality across the BRICS: an age-period-cohort analysis for the GBD 2019
Abstract
Background: Tuberculosis is the leading cause of death from a single infectious agent among the HIV-negative population and ranks first among the HIV-positive population. However, few studies have assessed tuberculosis trends in Brazil, Russia, India, China and South Africa (BRICS) or with an emphasis on HIV status. This study assesses the time trends of tuberculosis mortality across the BRICS with an emphasis on HIV status from 1990 to 2019.
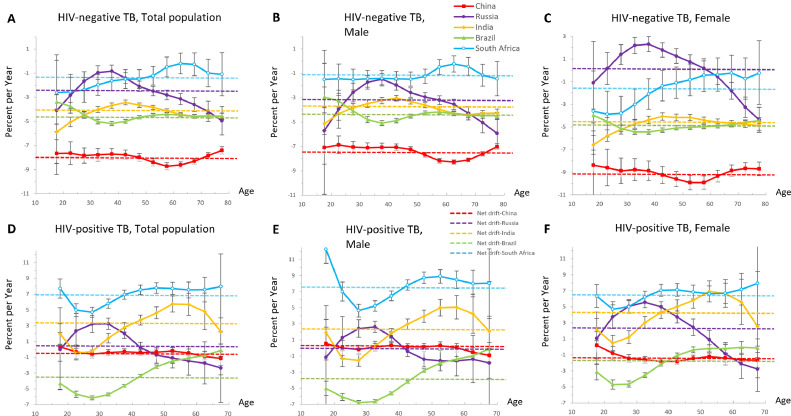
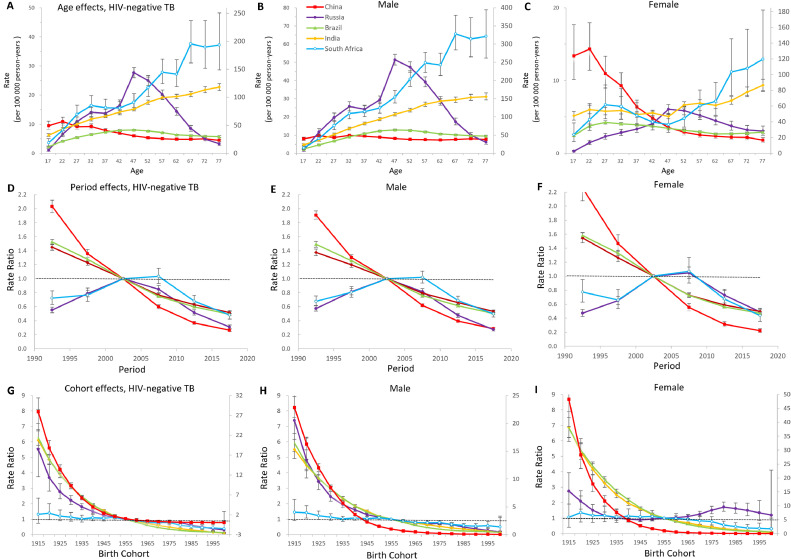
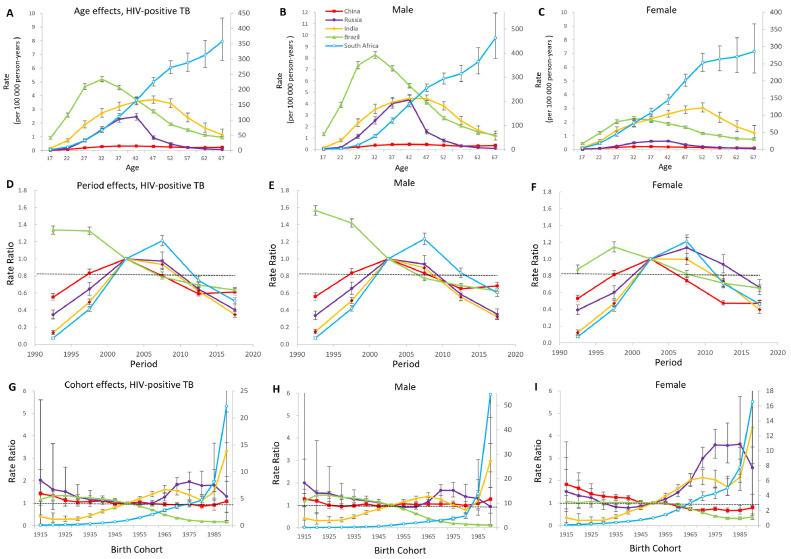
Methods: We obtained tuberculosis data from the Global Burden of Disease 2019 study (GBD 2019). We calculated the relative proportion of tuberculosis to all communicable, maternal, neonatal, and nutritional diseases by HIV status across the BRICS. We used age-period-cohort modelling to estimate cohort and period effects in tuberculosis from 1990 to 2019, and calculated net drift (overall annual percentage change), local drift (annual percentage change in each age group), longitudinal age curves (expected longitudinal age-specific rate), and period (cohort) relative risks.
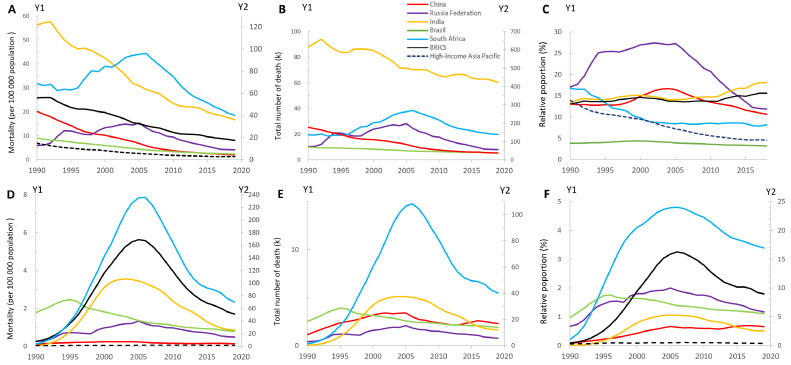
Findings: There were 549,522 tuberculosis deaths across the BRICS in 2019, accounting for 39.3% of global deaths. Among HIV-negative populations, the age-standardised mortality rate (ASMR) of tuberculosis in BRICS remained far higher than that of high-income Asia Pacific countries, especially in India (36.1 per 100 000 in 2019, 95% UI [30.7, 42.6]) and South Africa (40.1 per 100 000 in 2019, 95% UI [36.8, 43.7]). China had the fastest ASMR reduction across the BRICS, while India maintained the largest tuberculosis death numbers with an annual decrease much slower than China's (-4.1 vs -8.0%). Among HIV-positive populations, the ASMR in BRICS surged from 0.24 per 100 000 in 1990 to 5.63 per 100 000 in 2005, and then dropped quickly to 1.70 per 100 000 in 2019. Brazil was the first country to reverse the upward trend of HIV/AIDS-tuberculosis (HIV-TB) mortality in 1995, and achieved the most significant reduction (-3.32% per year). The HIV-TB mortality in South Africa has realised much progress since 2006, but still has the heaviest HIV-TB burden across the BRICS (ASMR: 70.0 per 100 000 in 2019). We also found unfavourable trends among HIV-negative middle-aged (35-55) adults of India, men over 50 in the HIV-negative population and whole HIV-positive population of South Africa, and women aged 45-55 years of Russia. China had little progress in its HIV-positive population with worsening period risks from 2010 to 2019, and higher risks in the younger cohorts born after 1980.
Interpretation: BRICS' actions on controlling tuberculosis achieved positive results, but the overall improvements were less than those in high-income Asia Pacific countries. BRICS and other high-burden countries should strengthen specified public health approaches and policies targeted at different priority groups in each country.
Funding: National Natural Science Foundation of China (82073573; 72074009), Peking University Global Health and Infectious Diseases Group.
Keywords: BRICS; HIV-negative; HIV-positive; Mortality; Tuberculosis.
© 2022 The Authors.
Conflict of interest statement
K Krishan reports non-financial support from the UGC Centre of Advanced Study (Phase II), Department of Anthropology, Panjab University, Chandigarh, India, outside the submitted work. Z Wang reports travel support from Bill & Melinda Gates Foundation for China-Gates TB project phase 3 in 2019. The other authors declare no competing interests.
Figures
References
-
- WHO . World Health Organization; Geneva: 2020. Global Tuberculosis Report 2020.
LinkOut - more resources
Full Text Sources
