

Neuroprotective effect of remote ischemic preconditioning in patients undergoing cardiac surgery: A randomized controlled trial
- PMID: 36148077
- PMCID: PMC9485807
- DOI: 10.3389/fcvm.2022.952033
Neuroprotective effect of remote ischemic preconditioning in patients undergoing cardiac surgery: A randomized controlled trial
Abstract
Background: The neuroprotective effect of remote ischemic preconditioning (RIPC) in patients undergoing elective cardiopulmonary bypass (CPB)-assisted coronary artery bypass graft (CABG) or valvular cardiac surgery remains unclear.
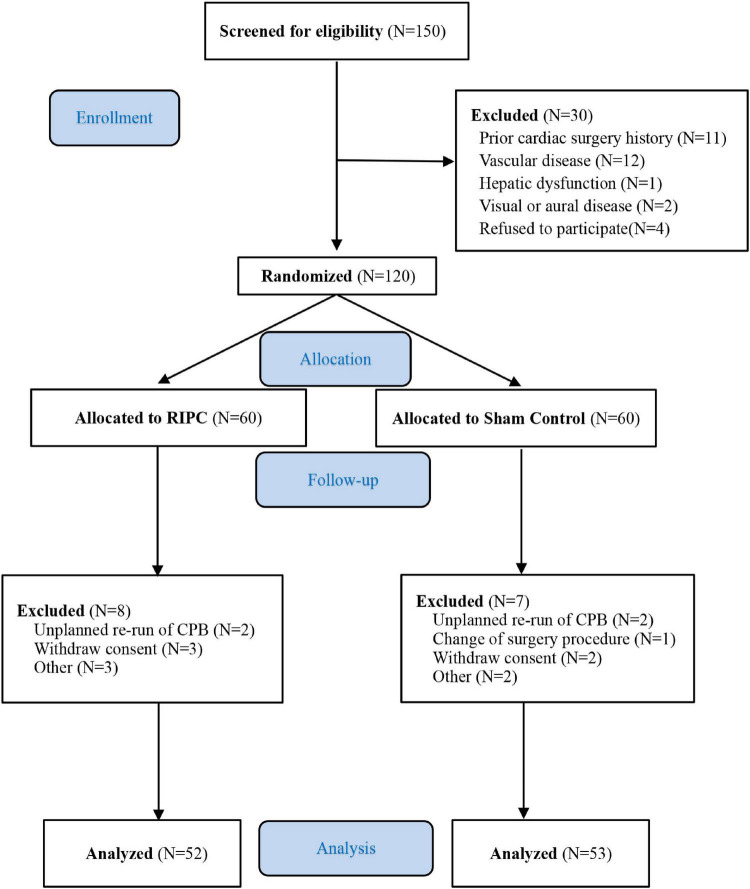
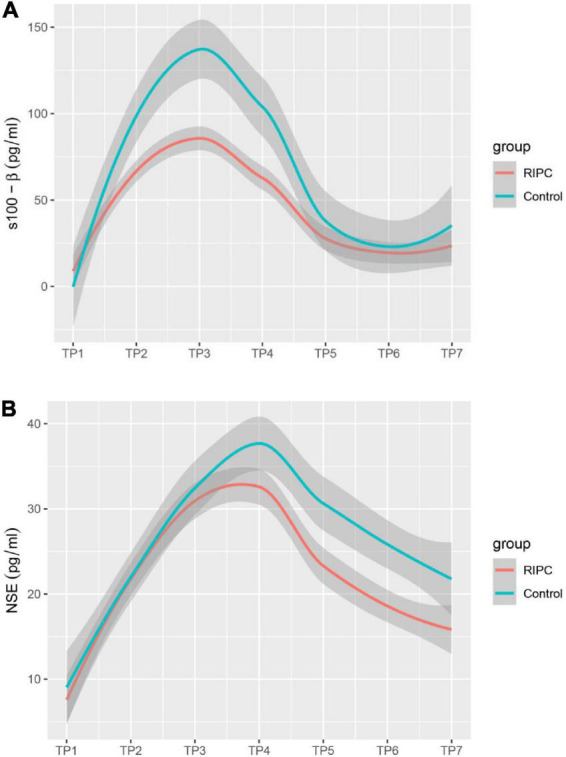
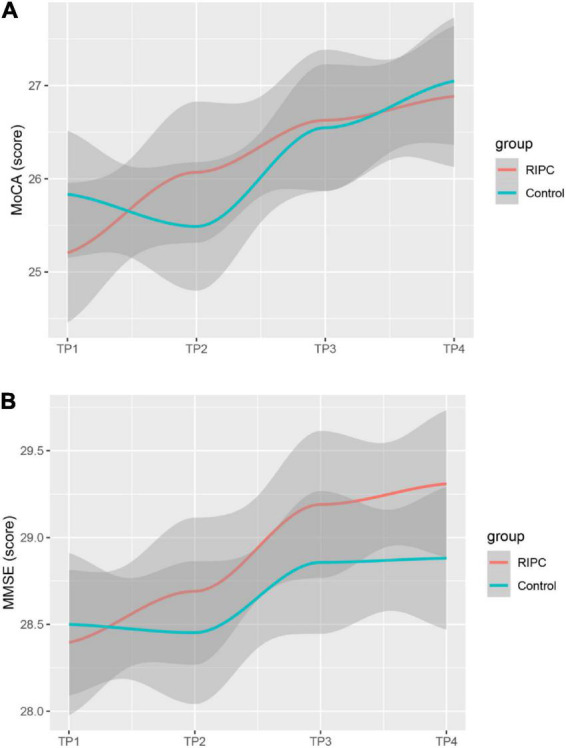
Methods: A randomized, double-blind, placebo-controlled superior clinical trial was conducted in patients undergoing elective on-pump coronary artery bypass surgery or valve surgery. Before anesthesia induction, patients were randomly assigned to RIPC (three 5-min cycles of inflation and deflation of blood pressure cuff on the upper limb) or the control group. The primary endpoint was the changes in S-100 calcium-binding protein β (S100-β) levels at 6 h postoperatively. Secondary endpoints included changes in Neuron-specific enolase (NSE), Mini-mental State Examination (MMSE), and Montreal Cognitive Assessment (MoCA) levels.
Results: A total of 120 patients [mean age, 48.7 years; 36 women (34.3%)] were randomized at three cardiac surgery centers in China. One hundred and five patients were included in the modified intent-to-treat analysis (52 in the RIPC group and 53 in the control group). The primary result demonstrated that at 6 h after surgery, S100-β levels were lower in the RIPC group than in the control group (50.75; 95% confidence interval, 67.08 to 64.40 pg/ml vs. 70.48; 95% CI, 56.84 to 84.10 pg/ml, P = 0.036). Compared to the control group, the concentrations of S100-β at 24 h and 72 h and the concentration of NSE at 6 h, 24 h, and 72 h postoperatively were significantly lower in the RIPC group. However, neither the MMSE nor the MoCA revealed significant between-group differences in postoperative cognitive performance at 7 days, 3 months, and 6 months after surgery.
Conclusion: In patients undergoing CPB-assisted cardiac surgery, RIPC attenuated brain damage as indicated with the decreased release of brain damage biomarker S100-β and NSE.
Clinical trial registration: [ClinicalTrials.gov], identifier [NCT01231789].
Keywords: cardiac surgery; neuroprotective effect; postoperative cognitive dysfunction; remote ischemic preconditioning; surrogate.
Copyright © 2022 Zhu, Zheng, Lv, Ouyang, Han, Zhang, Dong and Lei.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The clinical utility of remote ischemic preconditioning in protecting against cardiac surgery-associated acute kidney injury: A pilot randomized clinical trial.Adv Clin Exp Med. 2020 Feb;29(2):189-196. doi: 10.17219/acem/112610. Adv Clin Exp Med. 2020. PMID: 32091672 Clinical Trial.
-
Remote ischemic preconditioning prevents deterioration of short-term postoperative cognitive function after cardiac surgery using cardiopulmonary bypass: results of a pilot investigation.J Cardiothorac Vasc Anesth. 2015 Apr;29(2):382-8. doi: 10.1053/j.jvca.2014.07.012. Epub 2014 Nov 1. J Cardiothorac Vasc Anesth. 2015. PMID: 25440646 Clinical Trial.
-
Effect of remote ischaemic preconditioning on clinical outcomes in patients undergoing cardiac bypass surgery: a randomised controlled clinical trial.Heart. 2015 Feb;101(3):185-92. doi: 10.1136/heartjnl-2014-306178. Epub 2014 Sep 24. Heart. 2015. PMID: 25252696 Clinical Trial.
-
Effect of Remote Ischaemic preconditioning on Clinical outcomes in patients undergoing Coronary Artery bypass graft surgery (ERICCA study): a multicentre double-blind randomised controlled clinical trial.Southampton (UK): NIHR Journals Library; 2016 Jun. Southampton (UK): NIHR Journals Library; 2016 Jun. PMID: 27359023 Free Books & Documents. Review.
-
Clinical Outcomes of Remote Ischemic Preconditioning Prior to Cardiac Surgery: A Meta-Analysis of Randomized Controlled Trials.J Am Heart Assoc. 2017 Feb 20;6(2):e004666. doi: 10.1161/JAHA.116.004666. J Am Heart Assoc. 2017. PMID: 28219918 Free PMC article. Review.
Cited by
-
2024 EACTS/EACTAIC/EBCP Guidelines on cardiopulmonary bypass in adult cardiac surgery.Interdiscip Cardiovasc Thorac Surg. 2025 Feb 5;40(2):ivaf002. doi: 10.1093/icvts/ivaf002. Interdiscip Cardiovasc Thorac Surg. 2025. PMID: 39949317 Free PMC article. No abstract available.
-
2024 EACTS/EACTAIC/EBCP Guidelines on cardiopulmonary bypass in adult cardiac surgery.Br J Anaesth. 2025 Apr;134(4):917-1008. doi: 10.1016/j.bja.2025.01.015. Epub 2025 Feb 14. Br J Anaesth. 2025. PMID: 39955230 Free PMC article.
-
Communication Regarding the Myocardial Ischemia/Reperfusion and Cognitive Impairment: A Narrative Literature Review.J Alzheimers Dis. 2024;97(4):1545-1570. doi: 10.3233/JAD-230886. J Alzheimers Dis. 2024. PMID: 38277294 Free PMC article. Review.
-
Remote ischemic preconditioning and cognitive dysfunction following coronary artery bypass grafting: A systematic review and meta-analysis of randomized controlled trials.Saudi J Anaesth. 2024 Apr-Jun;18(2):187-193. doi: 10.4103/sja.sja_751_23. Epub 2024 Mar 14. Saudi J Anaesth. 2024. PMID: 38654856 Free PMC article.
-
Remote ischaemic preconditioning for transcatheter aortic valve replacement: a protocol for a systematic review with meta-analysis and trial sequential analysis.BMJ Open. 2024 Apr 25;14(4):e080200. doi: 10.1136/bmjopen-2023-080200. BMJ Open. 2024. PMID: 38670623 Free PMC article.
References
Associated data
LinkOut - more resources
Full Text Sources
Medical