

Neuroprotective effect of remote ischemic preconditioning in patients undergoing cardiac surgery: A randomized controlled trial
- PMID: 36148077
- PMCID: PMC9485807
- DOI: 10.3389/fcvm.2022.952033
Neuroprotective effect of remote ischemic preconditioning in patients undergoing cardiac surgery: A randomized controlled trial
Abstract
Background: The neuroprotective effect of remote ischemic preconditioning (RIPC) in patients undergoing elective cardiopulmonary bypass (CPB)-assisted coronary artery bypass graft (CABG) or valvular cardiac surgery remains unclear.
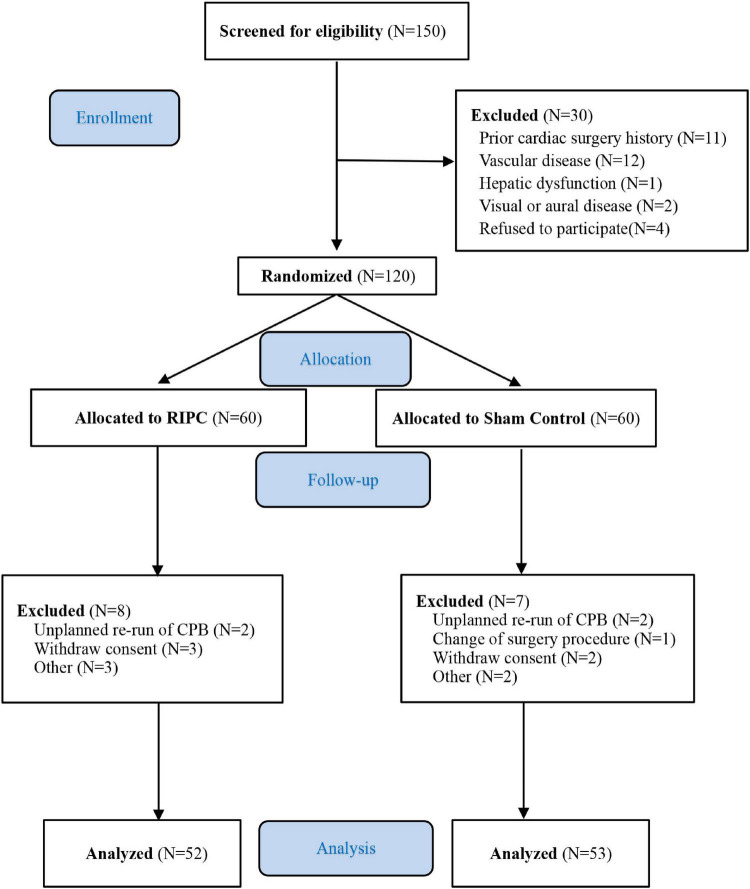
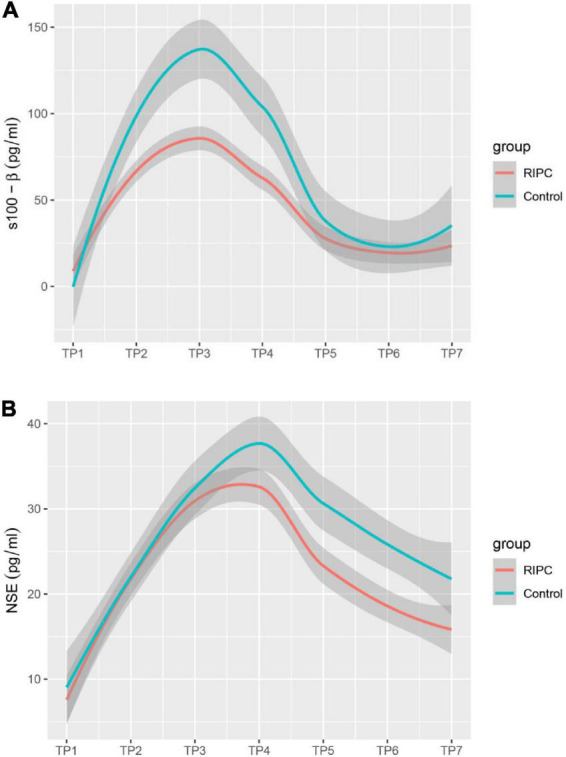
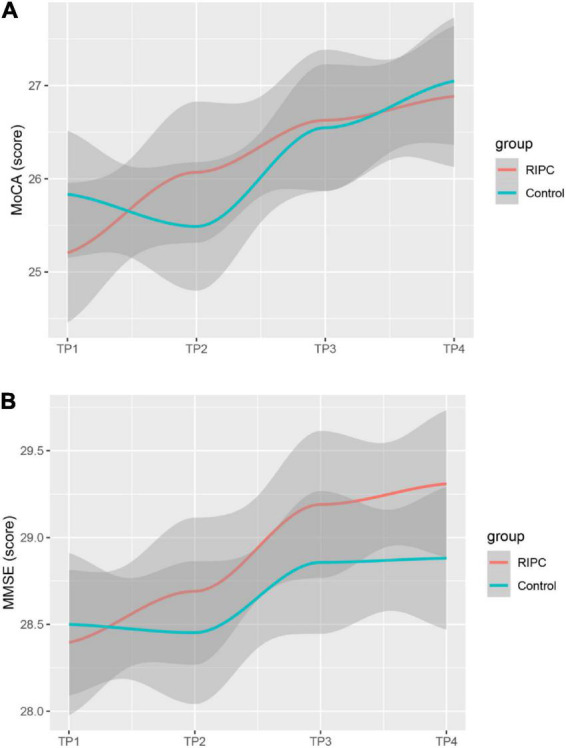
Methods: A randomized, double-blind, placebo-controlled superior clinical trial was conducted in patients undergoing elective on-pump coronary artery bypass surgery or valve surgery. Before anesthesia induction, patients were randomly assigned to RIPC (three 5-min cycles of inflation and deflation of blood pressure cuff on the upper limb) or the control group. The primary endpoint was the changes in S-100 calcium-binding protein β (S100-β) levels at 6 h postoperatively. Secondary endpoints included changes in Neuron-specific enolase (NSE), Mini-mental State Examination (MMSE), and Montreal Cognitive Assessment (MoCA) levels.
Results: A total of 120 patients [mean age, 48.7 years; 36 women (34.3%)] were randomized at three cardiac surgery centers in China. One hundred and five patients were included in the modified intent-to-treat analysis (52 in the RIPC group and 53 in the control group). The primary result demonstrated that at 6 h after surgery, S100-β levels were lower in the RIPC group than in the control group (50.75; 95% confidence interval, 67.08 to 64.40 pg/ml vs. 70.48; 95% CI, 56.84 to 84.10 pg/ml, P = 0.036). Compared to the control group, the concentrations of S100-β at 24 h and 72 h and the concentration of NSE at 6 h, 24 h, and 72 h postoperatively were significantly lower in the RIPC group. However, neither the MMSE nor the MoCA revealed significant between-group differences in postoperative cognitive performance at 7 days, 3 months, and 6 months after surgery.
Conclusion: In patients undergoing CPB-assisted cardiac surgery, RIPC attenuated brain damage as indicated with the decreased release of brain damage biomarker S100-β and NSE.
Clinical trial registration: [ClinicalTrials.gov], identifier [NCT01231789].
Keywords: cardiac surgery; neuroprotective effect; postoperative cognitive dysfunction; remote ischemic preconditioning; surrogate.
Copyright © 2022 Zhu, Zheng, Lv, Ouyang, Han, Zhang, Dong and Lei.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical