

Radiomics artificial intelligence modelling for prediction of local control for colorectal liver metastases treated with radiotherapy
- PMID: 36148155
- PMCID: PMC9485899
- DOI: 10.1016/j.phro.2022.09.004
Radiomics artificial intelligence modelling for prediction of local control for colorectal liver metastases treated with radiotherapy
Abstract
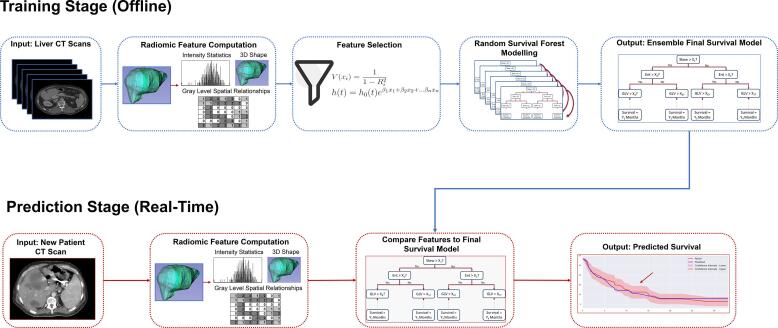
Background and purpose: Prognostic assessment of local therapies for colorectal liver metastases (CLM) is essential for guiding management in radiation oncology. Computed tomography (CT) contains liver texture information which may be predictive of metastatic environments. To investigate the feasibility of analyzing CT texture, we sought to build an automated model to predict progression-free survival using CT radiomics and artificial intelligence (AI).
Materials and methods: Liver CT scans and outcomes for N = 97 CLM patients treated with radiotherapy were retrospectively obtained. A survival model was built by extracting 108 radiomic features from liver and tumor CT volumes for a random survival forest (RSF) to predict local progression. Accuracies were measured by concordance indices (C-index) and integrated Brier scores (IBS) with 4-fold cross-validation. This was repeated with different liver segmentations and radiotherapy clinical variables as inputs to the RSF. Predictive features were identified by perturbation importances.
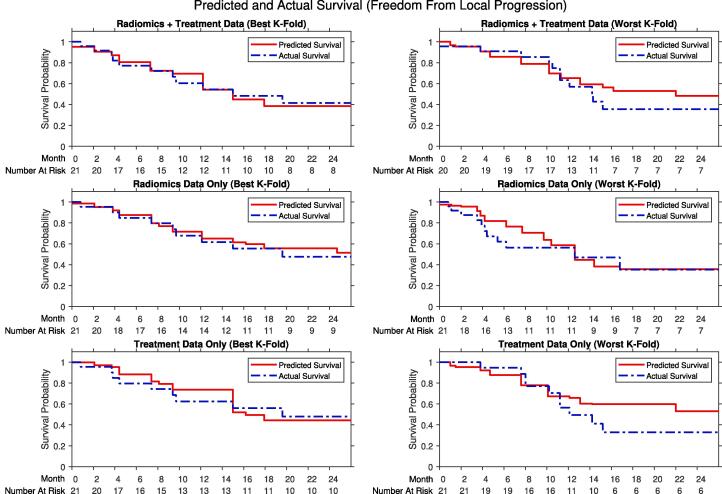
Results: The AI radiomics model achieved a C-index of 0.68 (CI: 0.62-0.74) and IBS below 0.25 and the most predictive radiomic feature was gray tone difference matrix strength (importance: 1.90 CI: 0.93-2.86) and most predictive treatment feature was maximum dose (importance: 3.83, CI: 1.05-6.62). The clinical data only model achieved a similar C-index of 0.62 (CI: 0.56-0.69), suggesting that predictive signals exist in radiomics and clinical data.
Conclusions: The AI model achieved good prediction accuracy for progression-free survival of CLM, providing support that radiomics or clinical data combined with machine learning may aid prognostic assessment and management.
Keywords: Artificial intelligence; Computer vision; Machine learning; Radiomics; Survival analysis.
© 2022 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Paul B. Romesser is a EMD Serono consultant and reports support for travel from Elekta and Philips healthcare and prior research funding from EMD Serono.
Figures
References
-
- Abdalla E.K., Vauthey J.N., Ellis L.M., Ellis V., Pollock R., Broglio K., et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Ann Surg. 2004;239:818–827. doi: 10.1097/01.sla.0000128305.90650.71. - DOI - PMC - PubMed
-
- Ruers T, Van Coevorden F, Punt CJ, Pierie JE, Borel-Rinkes I, Ledermann JA, et al. Local treatment of unresectable colorectal liver metastases: results of a randomized phase II trial. J Natl Cancer Inst. 2017;109:djx015. https://doi.org/10.1093/jnci/djx015. - PMC - PubMed
-
- Mahadevan A., Blanck O., Lanciano R., Peddada A., Sundararaman S., D'Ambrosio D., et al. Stereotactic Body Radiotherapy (SBRT) for liver metastasis - clinical outcomes from the international multi-institutional RSSearch® Patient Registry. Radiat Oncol. 2018;13:26. doi: 10.1186/s13014-018-0969-2. - DOI - PMC - PubMed
-
- Nordlinger B., Guiguet M., Vaillant J.C., Balladur P., Boudjema K., Bachellier P., et al. Surgical resection of colorectal carcinoma metastases to the liver. A prognostic scoring system to improve case selection, based on 1568 patients. Association Française de Chirurgie. Cancer. 1996;77:1254–1262. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
