

Critical success factors for high routine immunization performance: A case study of Nepal
- PMID: 36148265
- PMCID: PMC9486040
- DOI: 10.1016/j.jvacx.2022.100214
Critical success factors for high routine immunization performance: A case study of Nepal
Abstract
Introduction: The essential components of a vaccine delivery system are well-documented, but robust evidence on how and why the related processes and implementation strategies drive catalytic improvements in vaccination coverage are not well established. To address this gap, we identified critical success factors that may have led to substantial improvements in routine childhood immunization coverage in Nepal from 2000 through 2019.
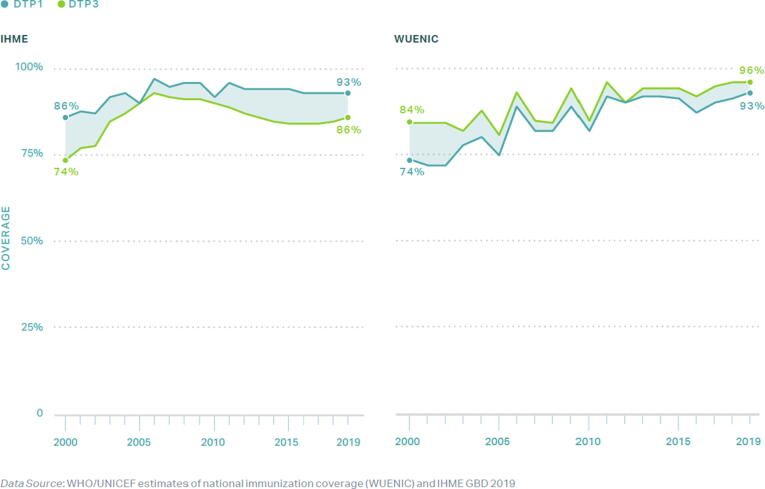
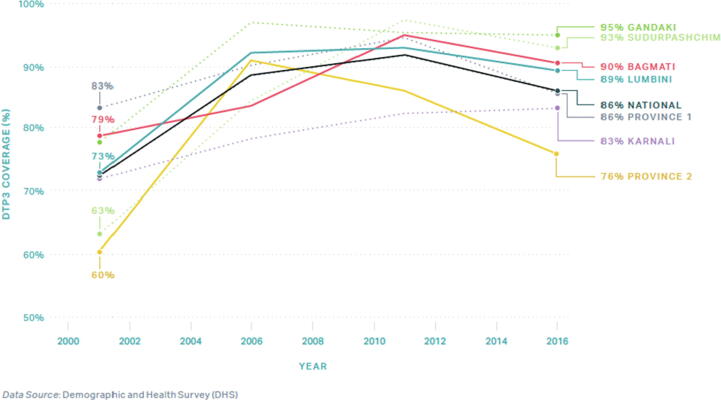
Methods: We identified Nepal as an exemplar in the delivery of early childhood immunization through analysis of DTP1 and DTP3 coverage data. Through interviews and focus group discussions at the national, regional, district, health post, and community level, we investigated factors that contributed to high and sustained vaccine coverage. We conducted a thematic analysis through application of implementation science frameworks to determine critical success factors. We triangulated these findings with quantitative analyses using publicly available data.
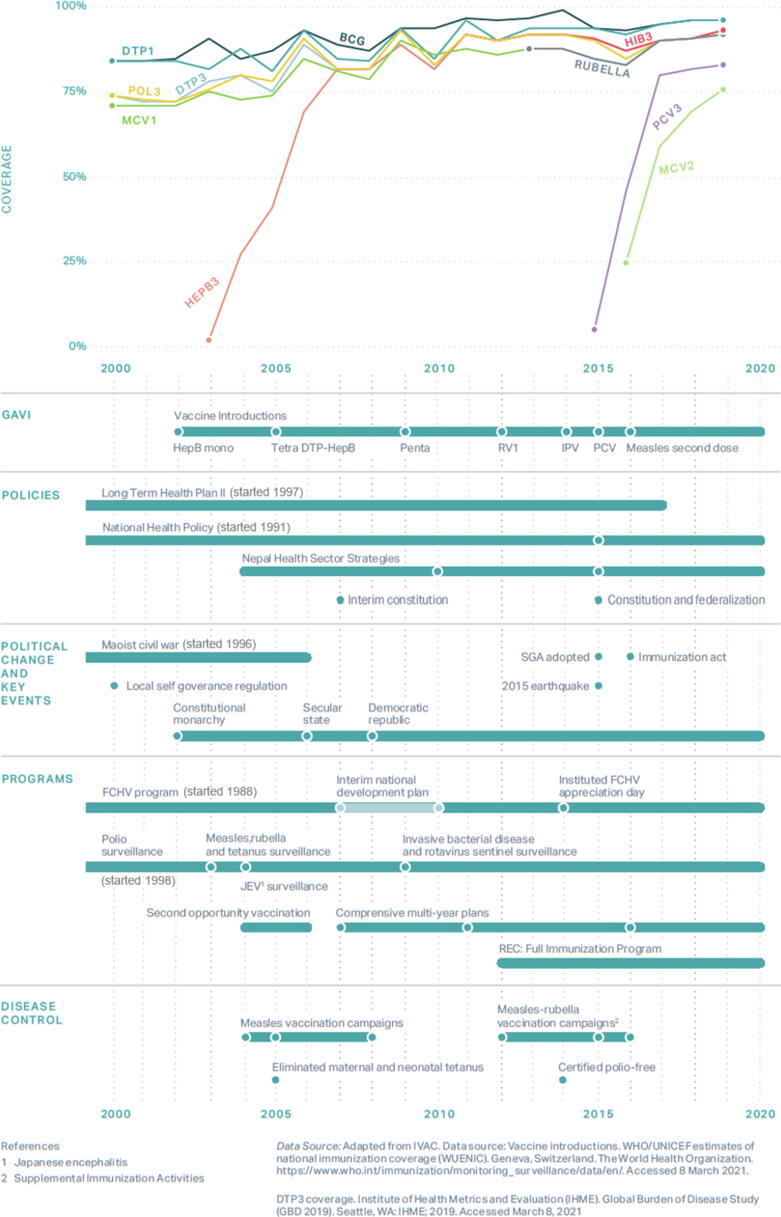
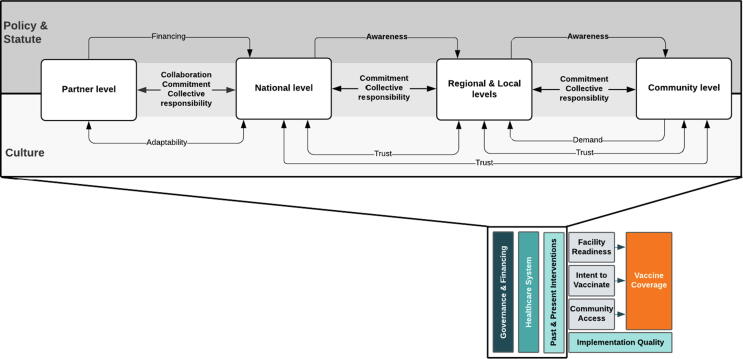
Results: The following success factors emerged: 1) Codification of health as a human right, - along with other vaccine-specific legislation - ensured the stability of vaccination programming; 2) National and multi-national partnerships supported information sharing, division of labor, and mutual capacity building; 3) Pro-vaccine messaging through various mediums, which was tailored to local needs, generated public awareness; 4) Female Community Health Volunteers educated community members as trusted and compassionate neighbors; and 5) Cultural values fostered collective responsibility and community ownership of vaccine coverage.
Conclusion: This case study of Nepal suggests that the success of its national immunization program relied on the engagement and understanding of the beneficiaries. The immunization program was supported by consistent and reliable commitment, collaboration, awareness, and collective responsibility between the government, community, and partners. These networks are strengthened through a collective dedication to vaccination programming and a universal belief in health as a human right.
Keywords: CHW, Community Health Worker; Childhood vaccination; DTP1, First dose of diphtheria-tetanus-pertussis containing vaccine; DTP3, Third dose ofdiphtheria-tetanus-pertussis containing vaccine; FCHV, Female Community Health Volunteer; GPEI, Global Polio Eradication Initiative; Health systems strengthening; Implementation research; MHG, Mother's Health Group; MoHP, Ministry of Health and Population; NHEICC, National Health Education Information and Communication Center; NIP, National Immunisation Programme; PEN, Polio Eradication Nepal; VDC, Village Development Committee; VPD, Vaccine Preventable Disease; Vaccine policy; Vaccine programming; WHO-IPD, World Health Organization - Immunization Preventable Diseases.
© 2022 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Jhalak Guatam is the head of the National Immunization Programme of Nepal - which was critically assessed for this study - and he received a full-time salary for that work. He served as a participant in this research with his data anonymized. The remaining authors have no conflicts of interest to declare.
Figures
Similar articles
-
Critical success factors for high routine immunization performance: A case study of Senegal.Vaccine X. 2023 Apr 6;14:100296. doi: 10.1016/j.jvacx.2023.100296. eCollection 2023 Aug. Vaccine X. 2023. PMID: 37113739 Free PMC article.
-
Success in vaccination programming through community health workers: a qualitative analysis of interviews and focus group discussions from Nepal, Senegal and Zambia.BMJ Open. 2024 Apr 3;14(4):e079358. doi: 10.1136/bmjopen-2023-079358. BMJ Open. 2024. PMID: 38569679 Free PMC article.
-
Critical success factors for routine immunization performance: A case study of Zambia 2000 to 2018.Vaccine X. 2022 Apr 30;11:100166. doi: 10.1016/j.jvacx.2022.100166. eCollection 2022 Aug. Vaccine X. 2022. PMID: 35707220 Free PMC article.
-
Strengthening vaccination policies in Latin America: an evidence-based approach.Vaccine. 2013 Aug 20;31(37):3826-33. doi: 10.1016/j.vaccine.2012.12.062. Epub 2013 Jan 25. Vaccine. 2013. PMID: 23357196 Review.
-
Pakistan's expanded programme on immunization: an overview in the context of polio eradication and strategies for improving coverage.Vaccine. 2013 Jul 18;31(33):3313-9. doi: 10.1016/j.vaccine.2013.05.015. Epub 2013 May 22. Vaccine. 2013. PMID: 23707167 Review.
Cited by
-
Critical success factors for high routine immunization performance: A case study of Senegal.Vaccine X. 2023 Apr 6;14:100296. doi: 10.1016/j.jvacx.2023.100296. eCollection 2023 Aug. Vaccine X. 2023. PMID: 37113739 Free PMC article.
-
Using the Journey to Health and Immunization (JTHI) Framework to Engage Stakeholders in Identifying Behavioral and Social Drivers of Routine Immunization in Nepal.Vaccines (Basel). 2023 Nov 10;11(11):1709. doi: 10.3390/vaccines11111709. Vaccines (Basel). 2023. PMID: 38006041 Free PMC article.
-
The COVID-19 Vaccination Rollout in Tanzania: The Role of Coordination in Its Success.Vaccines (Basel). 2025 Apr 30;13(5):484. doi: 10.3390/vaccines13050484. Vaccines (Basel). 2025. PMID: 40432096 Free PMC article.
-
Bridging Gaps in Vaccine Access and Equity: A Middle Eastern Perspective.Vaccines (Basel). 2025 Jul 29;13(8):806. doi: 10.3390/vaccines13080806. Vaccines (Basel). 2025. PMID: 40872893 Free PMC article. Review.
-
Success in vaccination programming through community health workers: a qualitative analysis of interviews and focus group discussions from Nepal, Senegal and Zambia.BMJ Open. 2024 Apr 3;14(4):e079358. doi: 10.1136/bmjopen-2023-079358. BMJ Open. 2024. PMID: 38569679 Free PMC article.
References
-
- World Health Organization, Immunization Agenda 2030: A Global Strategy to Leave No One Behind. 2020. - PubMed
-
- Vanderslott S., Dadonaite B., Roser M. Vaccination. 2013 Online.
-
- Piot P., et al. Immunization: vital progress, unfinished agenda. Nature. 2019;575(7781):119–129. - PubMed
-
- World Health Organization, Global Vaccine Action Plan 2011–2020 2013: USA.
-
- World Health Organization. Immunization coverage. 2020 July 15, 2020 August 4, 2020]; Available from: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage.
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
