

Novel TrueVue series of 3D echocardiography: Revealing the pathological morphology of congenital heart disease
- PMID: 36148295
- PMCID: PMC9485809
- DOI: 10.3389/fphys.2022.1000007
Novel TrueVue series of 3D echocardiography: Revealing the pathological morphology of congenital heart disease
Abstract
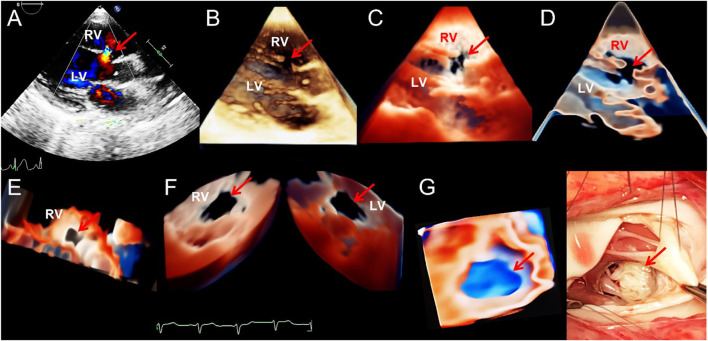
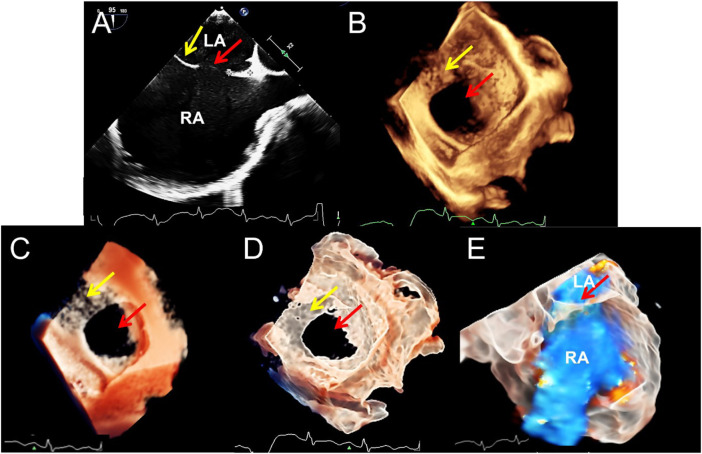
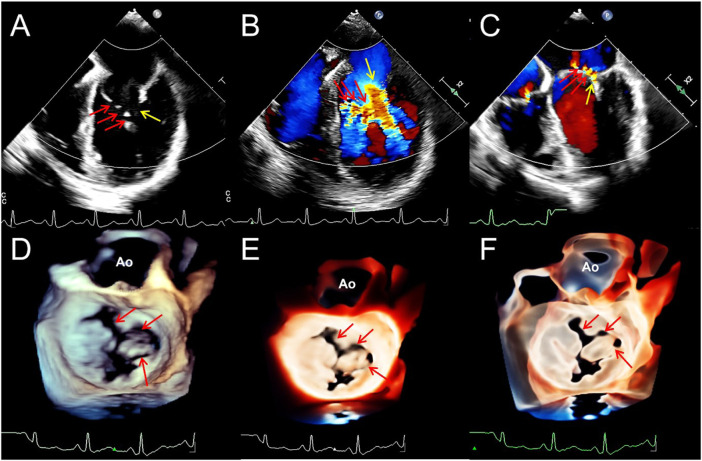
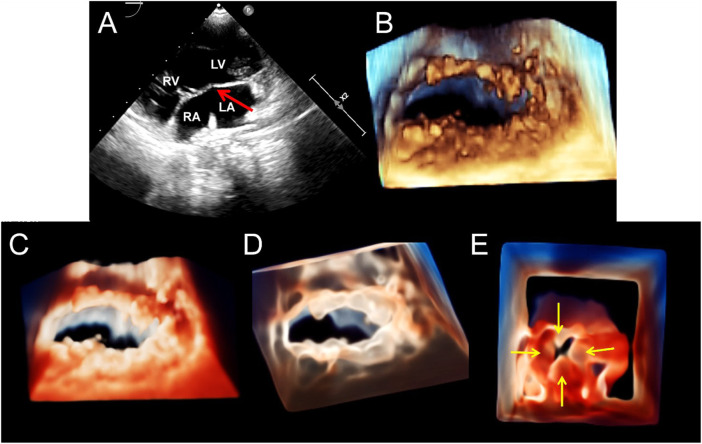
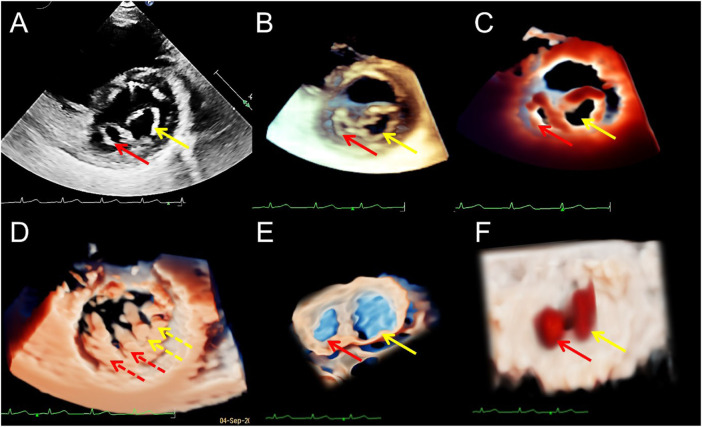
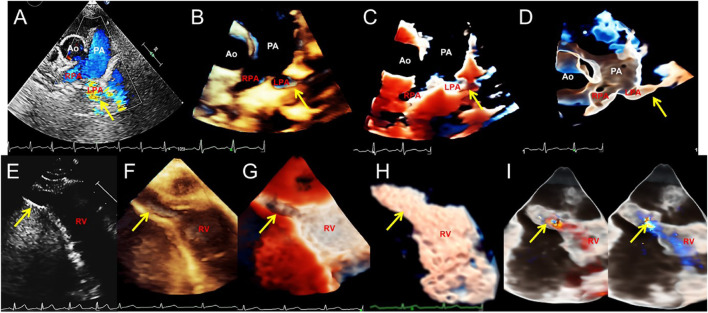
Aims: This study explored the advantages and limitations of novel series of three-dimensional (3D) echocardiographic techniques and summarized their application methods for congenital heart diseases (CHDs). Method and result: Two-dimensional (2D), traditional 3D echocardiography, and TrueVue plus light and/or Glass novel 3D technologies were performed on 62 patients with CHD, and a clinical survey was designed to judge whether the novel 3D images were more helpful for understanding the cardiac condition and guide treatment than traditional 3D images. TrueVue increased the visual resolution and simulated the true texture of cardiac tissue, significantly improving the display ability of abnormal anatomical structures in CHDs. TrueVue Glass displayed the blood channel and the internal structure of cardiac cavity more intuitively, indicating a new observation aspect not shown by conventional echocardiography. The clinical survey results showed that the new 3D imaging methods effectively increased the diagnostic confidence of echocardiographers, enabled surgeons to better understand the details of lesions, promoted efficient communication, and improved the confidence of both doctors and patients in treatment. Conclusion: The combined application of TrueVue, TrueVue Light, and TrueVue Glass more closely simulated real anatomical features, showed more comprehensive and subtle blood flow in the lumen, not only increased the visual effect but also provided more useful diagnostic information, improved the accuracy of evaluation and treatment of CHD when compared to traditional imaging techniques, indicating that this combined application has significant clinical value.
Keywords: congenital abnormalities; echocardiography; heart defects; real-time three-dimensional; ultrasonic imaging.
Copyright © 2022 Sun, Sun, Chen, Xiao, Zhang, Qiao, Tan, Liang, Li, Yang and Ren.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Anwar A. M., Soliman O., Bosch A. E. V. D., Mcghie J. S., Meijboom F. J., ten Cate F. J., et al. (2007). Assessment of pulmonary valve and right ventricular outflow tract with real-time three-dimensional echocardiography. Int. J. Cardiovasc. Imaging 23, 167–175. 10.1007/s10554-006-9142-3 - DOI - PubMed
LinkOut - more resources
Full Text Sources