

Innovative Designs and Logistical Considerations for Expedited Clinical Development of Combination Disease-Modifying Treatments for Type 1 Diabetes
- PMID: 36150059
- PMCID: PMC9911317
- DOI: 10.2337/dc22-0308
Innovative Designs and Logistical Considerations for Expedited Clinical Development of Combination Disease-Modifying Treatments for Type 1 Diabetes
Erratum in
-
Erratum. Innovative Designs and Logistical Considerations for Expedited Clinical Development of Combination Disease-Modifying Treatments for Type 1 Diabetes. Diabetes Care 2022;45:2189-2201.Diabetes Care. 2022 Dec 1;45(12):3113. doi: 10.2337/dc22-er12a. Diabetes Care. 2022. PMID: 36219765 Free PMC article. No abstract available.
Abstract
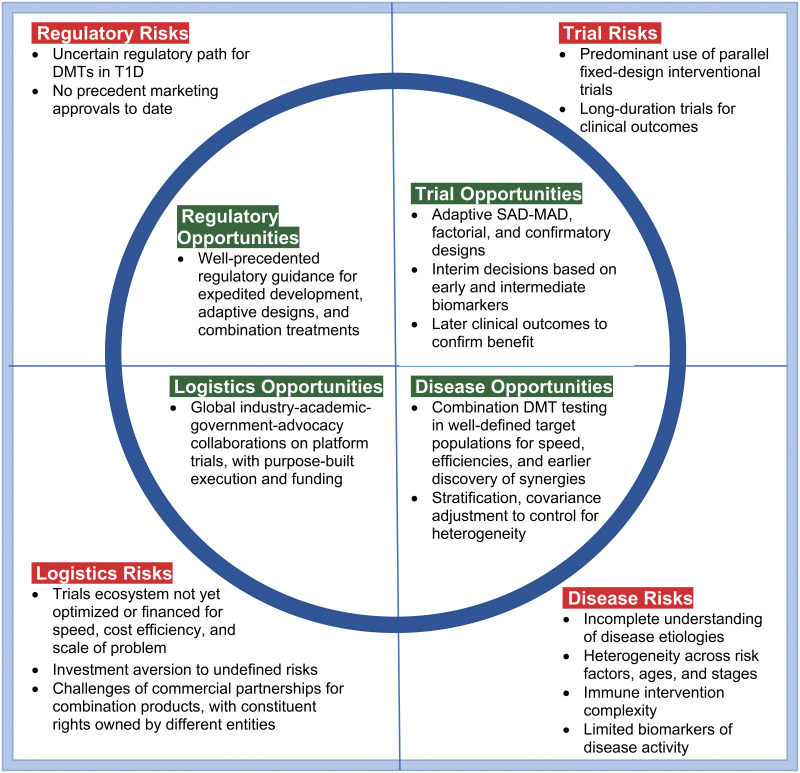
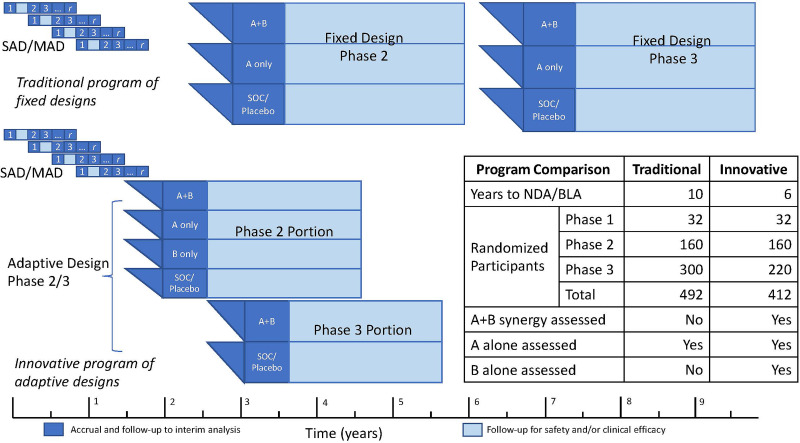
It has been 100 years since the life-saving discovery of insulin, yet daily management of type 1 diabetes (T1D) remains challenging. Even with closed-loop systems, the prevailing need for persons with T1D to attempt to match the kinetics of insulin activity with the kinetics of carbohydrate metabolism, alongside dynamic life factors affecting insulin requirements, results in the need for frequent interventions to adjust insulin dosages or consume carbohydrates to correct mismatches. Moreover, peripheral insulin dosing leaves the liver underinsulinized and hyperglucagonemic and peripheral tissues overinsulinized relative to their normal physiologic roles in glucose homeostasis. Disease-modifying therapies (DMT) to preserve and/or restore functional β-cell mass with controlled or corrected autoimmunity would simplify exogenous insulin need, thereby reducing disease mortality, morbidity, and management burdens. However, identifying effective DMTs for T1D has proven complex. There is some consensus that combination DMTs are needed for more meaningful clinical benefit. Other complexities are addressable with more innovative trial designs and logistics. While no DMT has yet been approved for marketing, existing regulatory guidance provides opportunities to further "de-risk" development. The T1D development ecosystem can accelerate progress by using more innovative ways for testing DMTs for T1D. This perspective outlines suggestions for accelerating evaluation of candidate T1D DMTs, including combination therapies, by use of innovative trial designs, enhanced logistical coordination of efforts, and regulatory guidance for expedited development, combination therapies, and adaptive designs.
© 2022 by the American Diabetes Association.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
