

A novel capnogram analysis to guide ventilation during cardiopulmonary resuscitation: clinical and experimental observations
- PMID: 36151559
- PMCID: PMC9508761
- DOI: 10.1186/s13054-022-04156-0
A novel capnogram analysis to guide ventilation during cardiopulmonary resuscitation: clinical and experimental observations
Abstract
Background: Cardiopulmonary resuscitation (CPR) decreases lung volume below the functional residual capacity and can generate intrathoracic airway closure. Conversely, large insufflations can induce thoracic distension and jeopardize circulation. The capnogram (CO2 signal) obtained during continuous chest compressions can reflect intrathoracic airway closure, and we hypothesized here that it can also indicate thoracic distension.
Objectives: To test whether a specific capnogram may identify thoracic distension during CPR and to assess the impact of thoracic distension on gas exchange and hemodynamics.
Methods: (1) In out-of-hospital cardiac arrest patients, we identified on capnograms three patterns: intrathoracic airway closure, thoracic distension or regular pattern. An algorithm was designed to identify them automatically. (2) To link CO2 patterns with ventilation, we conducted three experiments: (i) reproducing the CO2 patterns in human cadavers, (ii) assessing the influence of tidal volume and respiratory mechanics on thoracic distension using a mechanical lung model and (iii) exploring the impact of thoracic distension patterns on different circulation parameters during CPR on a pig model.
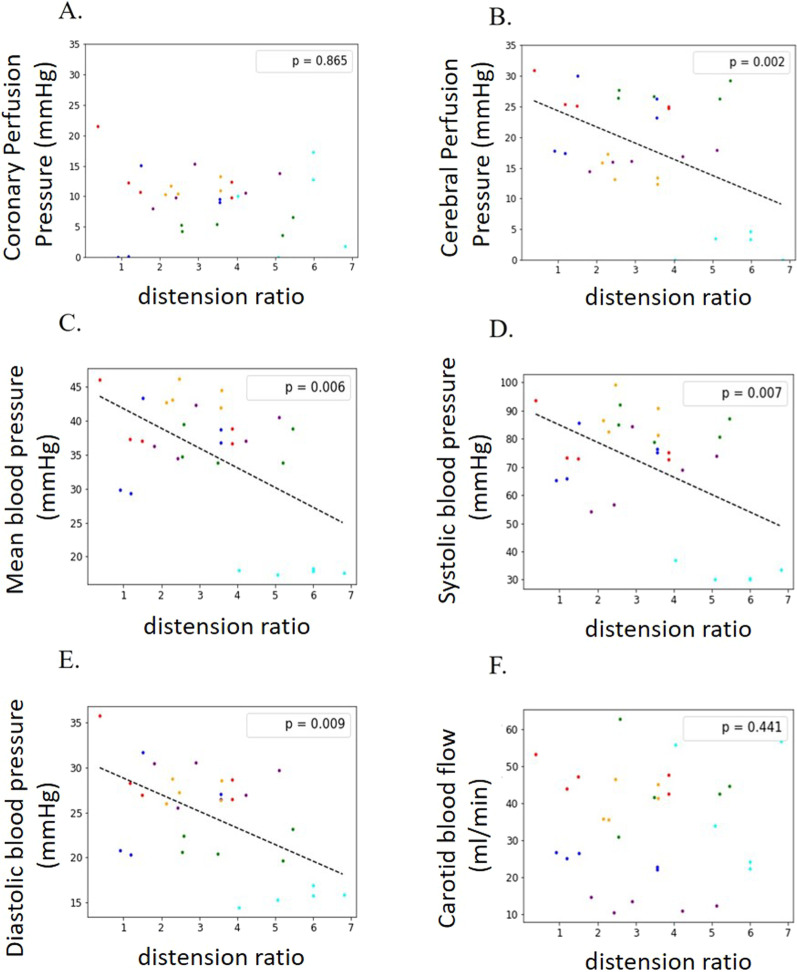
Measurements and main results: (1) Clinical data: 202 capnograms were collected. Intrathoracic airway closure was present in 35%, thoracic distension in 22% and regular pattern in 43%. (2) Experiments: (i) Higher insufflated volumes reproduced thoracic distension CO2 patterns in 5 cadavers. (ii) In the mechanical lung model, thoracic distension patterns were associated with higher volumes and longer time constants. (iii) In six pigs during CPR with various tidal volumes, a CO2 pattern of thoracic distension, but not tidal volume per se, was associated with a significant decrease in blood pressure and cerebral perfusion.
Conclusions: During CPR, capnograms reflecting intrathoracic airway closure, thoracic distension or regular pattern can be identified. In the animal experiment, a thoracic distension pattern on the capnogram is associated with a negative impact of ventilation on blood pressure and cerebral perfusion during CPR, not predicted by tidal volume per se.
Keywords: CO2 pattern; Cardiac arrest; Cardiopulmonary resuscitation; Intrathoracic airway closure; Thoracic distension.
© 2022. The Author(s).
Conflict of interest statement
AL is Ph.D. student in the Med2Lab partially funded by Air Liquide Medical Systems. DS reports grants from Fisher & Paykel and travel fees from Air Liquide Medical Systems. SD is consultant for Vitalaire Canada INC. FB reports personal fees from Löwenstein Medical, travel fees from Draeger and Air Liquide Medical systems and research support from Covidien, GE Healthcare and Getinge Group, outside this work. NP reports salary for research activities (Med2Lab) from Air Liquide Medical Systems. AB is master student from Telecom Physique Strasbourg University France. AM reports personal fees from Draeger, Faron Pharmaceuticals, Air Liquide Medical Systems, Pfizer, ResMed and Draeger and grants and personal fees from Fisher & Paykel and Covidien, outside this work. LB has received research grants for his research laboratory from Covidien (PAV), Draeger (EIT) and equipment from Fisher & Paykel (high flow), Air Liquide, Sentec (PtcCO2) and Philips (sleep) and received fees for lectures from Fisher & Paykel. RT reports grants from Air Liquide and grants, shares and personal fees from Orixha, all outside of this work. JCR reports part-time salary for research activities (Med2Lab) from Air Liquide Medical Systems and Vygon and grants from Creative Air Liquide. All other authors declare no competing interests.
Figures





References
-
- Leturiondo M, Ruiz de Gauna S, Ruiz JM, Julio Gutiérrez J, Leturiondo LA, González-Otero DM, et al. Influence of chest compression artefact on capnogram-based ventilation detection during out-of-hospital cardiopulmonary resuscitation. Resuscitation. 2018;124:63–68. doi: 10.1016/j.resuscitation.2017.12.013. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
