

Contrast-enhanced lymphatic US can improve the preoperative diagnostic performance for sentinel lymph nodes in early breast cancer
- PMID: 36152038
- PMCID: PMC9510155
- DOI: 10.1007/s00330-022-09139-x
Contrast-enhanced lymphatic US can improve the preoperative diagnostic performance for sentinel lymph nodes in early breast cancer
Abstract
Objectives: To evaluate the preoperative diagnostic value of contrast-enhanced lymphatic ultrasound (CEUS) for the sentinel lymph node (SLN) status in early breast cancer.
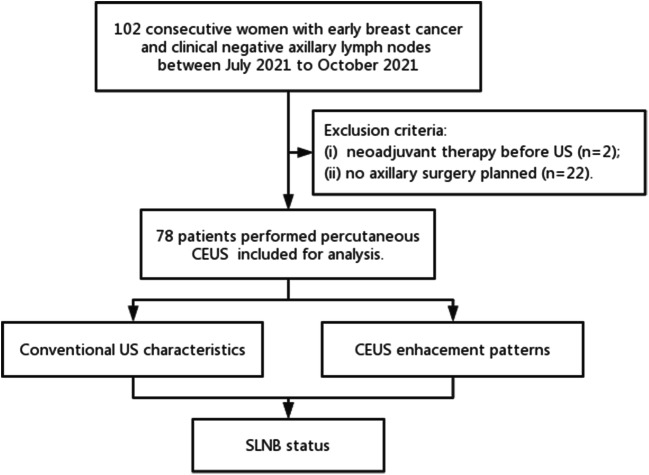
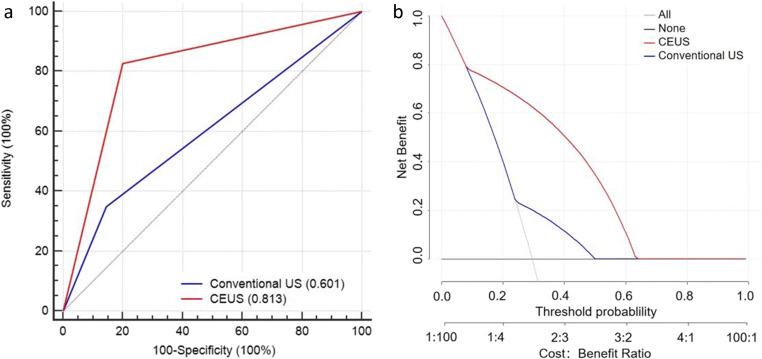
Materials and methods: We prospectively recruited 102 consecutive patients with clinically node-negative early breast cancer from July 2021 to October 2021. All patients underwent conventional US and percutaneous CEUS examinations. The CEUS of SLNs were classified into four enhancement patterns: homogeneous (I), featured inhomogeneous (II), focal defect (III), and no enhancement (IV). The diagnostic performance of conventional US and CEUS for SLN metastasis was assessed by receiver operating characteristic (ROC) curves and decision curves.
Results: A total of 78 women were enrolled in this study, including 55, 18, and 5 patients with negative axilla, 1-2, and ≥ 3 metastastic SLNs pathologically, respectively. The identification rate of SLNs by CEUS was 100%. Patterns I and II can select 91.7% (44/48) of patients with disease-free axilla, while patterns III and IV had higher percentages of metastasis (65.2%, p < 0.001 and 57.1%, p < 0.002, respectively). For the SLN metastatic burden, 100% (48/48) of patients with pattern I/II had ≤ 2 metastatic SLNs. Compared with conventional US, the CEUS enhancement patterns showed significant improvement in diagnosing metastatic SLNs (0.813 vs 0.601, p < 0.001). CEUS had greater clinical benefits and correctly reclassified 48% of metastatic SLNs (p < 0.001) without sacrificing the classification accuracy of negative SLNs (p = 0.25), and could improve prediction accuracy by 0.42 (p < 0.001).
Conclusions: CEUS demonstrated better diagnostic performance and greater clinical benefits than conventional US for the preoperative diagnosis of SLNs, showing its potential to select candidates for precluding axillary surgery in early breast cancer.
Key points: • The homogeneous and featured inhomogeneous enhancement of SLNs are highly suggestive of negative LNs, while focal defect (p < 0.001) and no enhancement (p < 0.002) patterns had higher percentages of metastasis. • The proportion of SLNs with highly suspicious signs on conventional US increases as the type of enhancement pattern increases (no suspicious signs in pattern I/II, 34.8% in pattern III, and 85.7% in pattern IV). • Compared with conventional US, CEUS improved the area under the receiver operating characteristic curve (0.813 vs. 0.601, p < 0.001) and had greater clinical benefits (IDI = 0.42, p < 0.001) for the diagnosis of axillary metastasis.
Keywords: Breast neoplasms; Contrast media; Sentinel lymph node; Ultrasonography.
© 2022. The Author(s), under exclusive licence to European Society of Radiology.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures

Similar articles
-
The Value of Percutaneous Contrast-Enhanced Ultrasound in Sentinel Lymph Node Identification, Metastatic Status and Burden Diagnosis in Early Breast Cancer.J Ultrasound Med. 2024 Feb;43(2):293-303. doi: 10.1002/jum.16359. Epub 2023 Oct 24. J Ultrasound Med. 2024. PMID: 37876335
-
Percutaneous contrast-enhanced ultrasound for localization and diagnosis of sentinel lymph node in early breast cancer.Sci Rep. 2019 Sep 19;9(1):13545. doi: 10.1038/s41598-019-49736-3. Sci Rep. 2019. PMID: 31537856 Free PMC article.
-
The value of contrast-enhanced ultrasound for sentinel lymph node identification and characterisation in pre-operative breast cancer patients: A prospective study.Eur Radiol. 2018 Apr;28(4):1654-1661. doi: 10.1007/s00330-017-5089-0. Epub 2017 Oct 20. Eur Radiol. 2018. PMID: 29058028
-
Accuracy of CEUS-guided sentinel lymph node biopsy in early-stage breast cancer: a study review and meta-analysis.World J Surg Oncol. 2020 May 29;18(1):112. doi: 10.1186/s12957-020-01890-z. World J Surg Oncol. 2020. PMID: 32471428 Free PMC article. Review.
-
How Pre-operative Sentinel Lymph Node Contrast-Enhanced Ultrasound Helps Intra-operative Sentinel Lymph Node Biopsy in Breast Cancer: Initial Experience.Ultrasound Med Biol. 2019 Aug;45(8):1865-1873. doi: 10.1016/j.ultrasmedbio.2019.04.006. Epub 2019 May 14. Ultrasound Med Biol. 2019. PMID: 31101445 Review.
Cited by
-
Diagnostic value of contrast-enhanced ultrasound for sentinel lymph node metastasis in breast cancer: an updated meta-analysis.Breast Cancer Res Treat. 2023 Nov;202(2):221-231. doi: 10.1007/s10549-023-07063-2. Epub 2023 Jul 27. Breast Cancer Res Treat. 2023. PMID: 37500963 Review.
-
Current status and future perspectives of contrast-enhanced ultrasound diagnosis of breast lesions.J Med Ultrason (2001). 2024 Oct;51(4):611-625. doi: 10.1007/s10396-024-01486-0. Epub 2024 Aug 23. J Med Ultrason (2001). 2024. PMID: 39174799 Free PMC article. Review.
-
Diagnostic value of different contrast-enhanced ultrasound (CEUS) methods for sentinel lymph node metastasis in patients with breast neoplasms: a meta-analysis and indirect comparison.Quant Imaging Med Surg. 2025 Jun 6;15(6):5660-5673. doi: 10.21037/qims-24-317. Epub 2025 Jun 3. Quant Imaging Med Surg. 2025. PMID: 40606373 Free PMC article.
-
Using four-point subcutaneous injection of lymphatic contrast-enhanced ultrasound to diagnose lymphedema of lower extremity.Quant Imaging Med Surg. 2024 Jul 1;14(7):4965-4971. doi: 10.21037/qims-24-300. Epub 2024 Jun 18. Quant Imaging Med Surg. 2024. PMID: 39022263 Free PMC article.
-
Super-resolution ultrasound imaging of intranodal lymphatic sinuses for predicting sentinel lymph node metastasis in breast cancer: a preliminary study.Eur Radiol. 2025 Apr 5. doi: 10.1007/s00330-025-11520-5. Online ahead of print. Eur Radiol. 2025. PMID: 40186632
References
-
- Giuliano AE, Ballman KV, McCall L, et al. Effect of axillary dissection vs no axillary dissection on 10-year overall survival among women with invasive breast cancer and sentinel node metastasis: the ACOSOG Z0011 (Alliance) randomized clinical trial. JAMA. 2017;318(10):918–926. doi: 10.1001/jama.2017.11470. - DOI - PMC - PubMed
-
- Krag DN, Anderson SJ, Julian TB, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 2010;11:927–933. doi: 10.1016/S1470-2045(10)70207-2. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
