

Surgery for brain metastases: radiooncology scores predict survival-score index for radiosurgery, graded prognostic assessment, recursive partitioning analysis
- PMID: 36152217
- PMCID: PMC9840567
- DOI: 10.1007/s00701-022-05356-x
Surgery for brain metastases: radiooncology scores predict survival-score index for radiosurgery, graded prognostic assessment, recursive partitioning analysis
Abstract
Background: Radiooncological scores are used to stratify patients for radiation therapy. We assessed their ability to predict overall survival (OS) in patients undergoing surgery for metastatic brain disease.
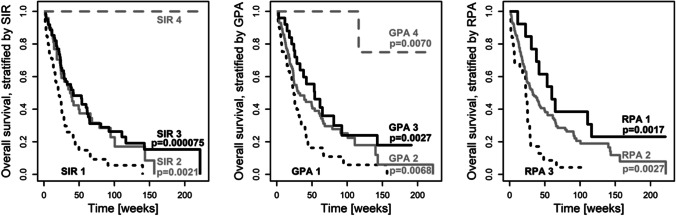
Methods: We performed a post-hoc single-center analysis of 175 patients, prospectively enrolled in the MetastaSys study data. Score index of radiosurgery (SIR), graded prognostic assessment (GPA), and recursive partitioning analysis (RPA) were assessed. All scores consider age, systemic disease, and performance status prior to surgery. Furthermore, GPA and SIR include the number of intracranial lesions while SIR additionally requires metastatic lesion volume. Predictive values for case fatality at 1 year after surgery were compared among scoring systems.
Results: All scores produced accurate reflections on OS after surgery (p ≤ 0.003). Median survival was 21-24 weeks in patients scored in the unfavorable cohorts, respectively. In cohorts with favorable scores, median survival ranged from 42 to 60 weeks. Favorable SIR was associated with a hazard ratio (HR) of 0.44 [0.29, 0.66] for death within 1 year. For GPA, the HR amounted to 0.44 [0.25, 0.75], while RPA had a HR of 0.30 [0.14, 0.63]. Overall test performance was highest for the SIR.
Conclusions: All scores proved useful in predicting OS. Considering our data, we recommend using the SIR for preoperative prognostic evaluation and counseling.
Keywords: Cerebral metastasis; Neurooncology; Scores; Surgery for brain tumors; Survival.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Agboola O, Benoit B, Cross P, et al. Prognostic factors derived from recursive partition analysis (RPA) of radiation therapy oncology group (RTOG) brain metastases trials applied to surgically resected and irradiated brain metastatic cases. Int J Radiat Oncol. 1998;42(1):155–159. doi: 10.1016/S0360-3016(98)00198-9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
