

Early antibiotic therapy is associated with a lower probability of successful liberation from mechanical ventilation in patients with severe acute exacerbation of chronic obstructive pulmonary disease
- PMID: 36153438
- PMCID: PMC9509513
- DOI: 10.1186/s13613-022-01060-2
Early antibiotic therapy is associated with a lower probability of successful liberation from mechanical ventilation in patients with severe acute exacerbation of chronic obstructive pulmonary disease
Abstract
Background: While antibiotic therapy is advocated to improve outcomes in acute exacerbation of chronic obstructive pulmonary disease (AECOPD) whenever mechanical ventilation is required, the evidence relies on small studies carried out before the era of widespread antibiotic resistance. Furthermore, the impact of systematic antibiotic therapy on successful weaning from mechanical ventilation was never investigated accounting for the competitive risk of death. The aim of the study was to assess whether early antibiotic therapy (eABT) increases successful mechanical ventilation weaning probability as compared to no eABT, in patients with AECOPD without pneumoniae, using multivariate competitive risk regression.
Methods: Retrospective analysis of patients admitted in 2 intensive care units (ICU) from 2012 to 2020 for AECOPD without pneumonia and requiring mechanical ventilation. eABT was defined as any anti-bacterial chemotherapy introduced during the first 24 h after ICU admission. The primary outcomes were the adjusted subdistribution hazard ratio (SHR) of the probability of being successfully weaned from mechanical ventilation (i.e. non-invasive and invasive ventilation) according to eABT status and accounting for the competitive risk of death.
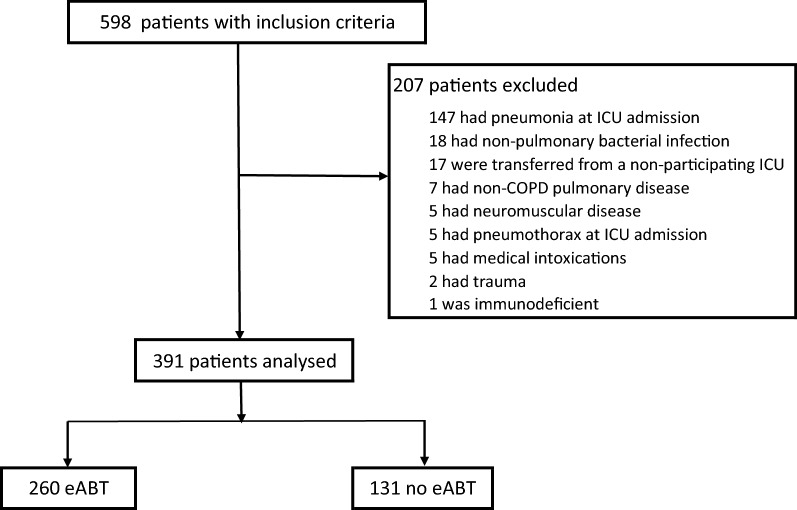
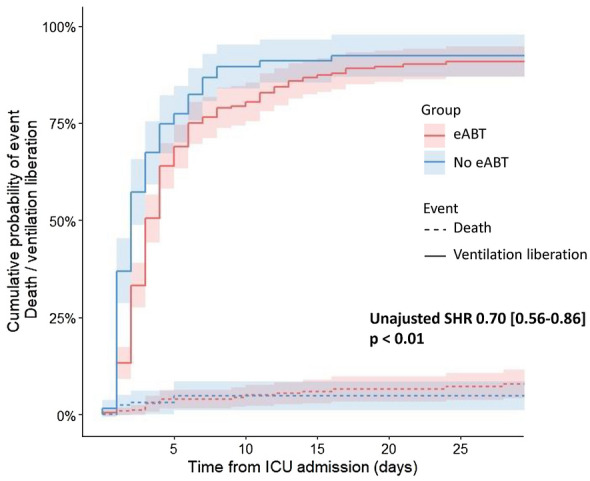
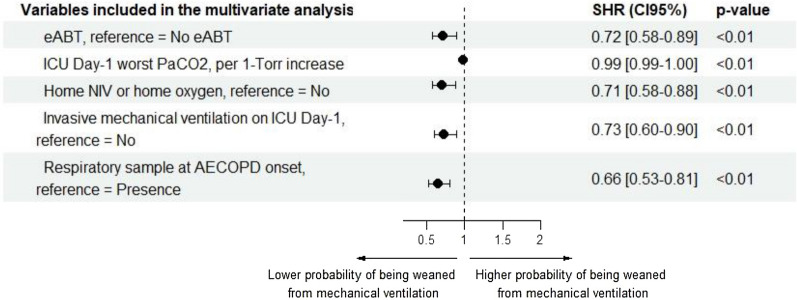
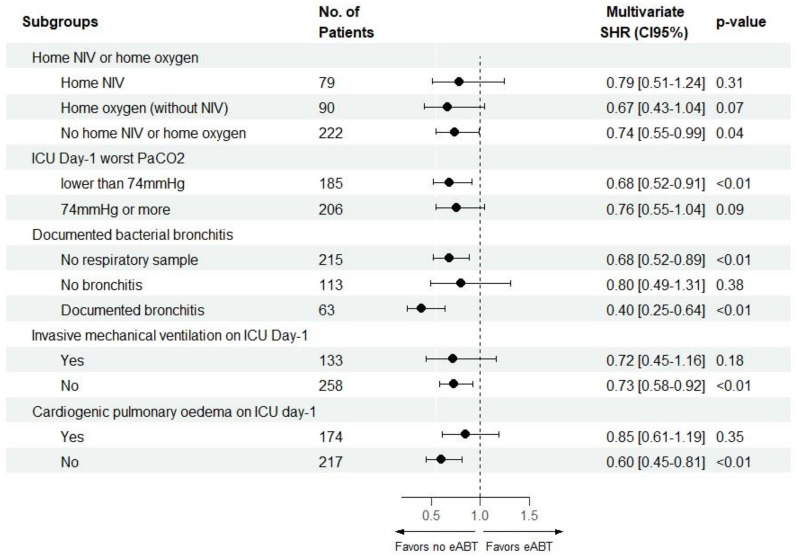
Results: Three hundred and ninety-one patients were included, of whom 66% received eABT. eABT was associated with a lower probability of successful liberation from mechanical ventilation when accounting for the competing risk of death in multivariate analyses (SHR 0.71 [95% confidence interval, 0.57-0.89], p < 0.01), after adjustment with covariates of disease severity. This association was present in all subgroups except in patients under invasive mechanical ventilation on ICU day-1, in patients with ICU day-1 worst PaCO2 > 74 torr (median value) and in patients with a documented bacterial bronchitis at ICU admission. Ventilator-free days at day 28, ICU-free days at day 28 and invasive mechanical ventilation-free days at day 28, were significantly lower in the eABT group, while there was no significant difference in mortality at day 28 between patients who received eABT and those who did not.
Conclusions: eABT was independently associated with a lower probability of being successfully weaned from mechanical ventilation, suggesting that the clinician decision to overrule systematic administration of eABT was not associated with a detectable harm in AECOPD ICU patients without pneumonia.
Keywords: Acute exacerbation; COPD; Chronic obstructive pulmonary disease; Mechanical ventilation; Ventilation weaning.
© 2022. The Author(s).
Conflict of interest statement
All authors, except one, have declared no conflicts of interest, financial or otherwise. JCR reported study funding by Hamilton Medical (Suisse) and a lecture compensated by Gilead Sciences (France), unrelated to the present work.
Figures
Similar articles
-
[Analysis of clinical effects of early enteral nutrition standardized treatment process management on patients with acute exacerbation of chronic obstructive pulmonary disease on invasive mechanical ventilation].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Jan;32(1):67-71. doi: 10.3760/cma.j.cn121430-20190927-00012. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32148234 Chinese.
-
[A multicenter study of respiratory multiple index in predicting weaning from mechanical ventilation in patients with acute exacerbation of chronic obstructive pulmonary disease].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2013 Jun;25(6):339-42. doi: 10.3760/cma.j.issn.2095-4352.2013.06.006. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2013. PMID: 23739566 Chinese.
-
Acute respiratory failure requiring mechanical ventilation in severe chronic obstructive pulmonary disease (COPD).Medicine (Baltimore). 2018 Apr;97(17):e0487. doi: 10.1097/MD.0000000000010487. Medicine (Baltimore). 2018. PMID: 29703009 Free PMC article.
-
COPD Exacerbation: Why It Is Important to Avoid ICU Admission.J Clin Med. 2023 May 9;12(10):3369. doi: 10.3390/jcm12103369. J Clin Med. 2023. PMID: 37240474 Free PMC article. Review.
-
Acute exacerbations of chronic obstructive pulmonary disease: diagnosis, management, and prevention in critically ill patients.Pharmacotherapy. 2015 Jun;35(6):631-48. doi: 10.1002/phar.1599. Epub 2015 Jun 1. Pharmacotherapy. 2015. PMID: 26032691 Review.
Cited by
-
The association between stress hyperglycemia and poor outcome in critically ill children is modulated by hyperlactatemia.Front Endocrinol (Lausanne). 2025 Jun 18;16:1518746. doi: 10.3389/fendo.2025.1518746. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40607229 Free PMC article.
References
-
- Forum of International Respiratory Societies. The Global Impact of Respiratory Disease – Second Edition. Sheffield, European Respiratory Society, 2017.
LinkOut - more resources
Full Text Sources
