

Computer grading of lung disease severity in patients with lymphangioleiomyomatosis referred for transplantation
- PMID: 36153516
- PMCID: PMC9509628
- DOI: 10.1186/s12890-022-02123-7
Computer grading of lung disease severity in patients with lymphangioleiomyomatosis referred for transplantation
Abstract
Objectives: Lymphangioleiomyomatosis (LAM) patients with severe lung disease may be considered for lung transplantation. Clinical, physiologic, and quality of life data are usually employed for referral. The aim of this study was to determine whether computed tomographic measurement of lung volume occupied by cysts (cyst score) complemented clinical and physiologic data in supporting referral for transplantation.
Methods: Forty-one patients were studied. Pre-referral clinical data, pulmonary function tests, exercise testing, and high-resolution computed tomography (HRCT) scans were obtained. From HRCT, a computer-aided diagnostic program was employed to calculate cyst scores. These data were compared to those of 41 age-matched LAM patients not referred for lung transplantation.
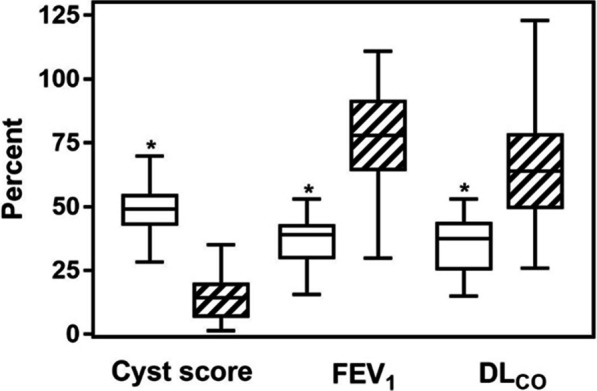
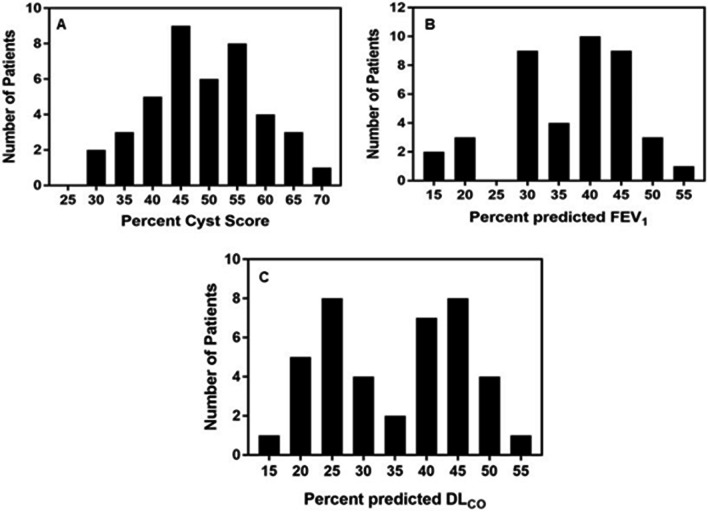
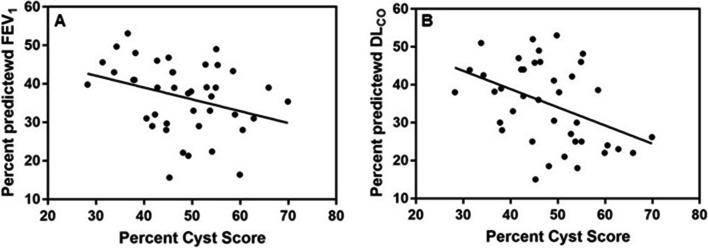
Results: Cyst score, and % predicted FEV1 and DLCO were respectively, 48.1 ± 9.4%, 36.5 ± 9.1%, and 35.0 ± 10.7%. For the control group, cyst score, FEV1, and DLCO were respectively, 14.8 ± 8.3%, 77.2 ± 20.3%, and 66.7 ± 19.3%. Cyst score values showed a normal distribution. However, the frequency distribution of FEV1 was skewed to the right while the distribution of DLCO was bimodal. Correlations between cyst score and FEV1 and DLCO for the study group were respectively, r = - 0.319 and r = - 0.421.
Conclusions: LAM patients referred for lung transplantation had nearly 50% of lungs occupied by cysts. Correlations between cyst score and FEV1 or DLCO were weak; as shown previously, DLCO was better related to cyst number while FEV1 had a better association with cyst size. Given its normal distribution, cyst score measurements may assist in evaluation of pre-transplant severity of lung disease before referral for transplantation.
Keywords: Cystic lung disease; High resolution computed tomography (HRCT); Lung transplant; Lymphangioleiomyomatosis (LAM).
© 2022. The Author(s).
Conflict of interest statement
None of the authors has any financial conflicts of interest
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
