Medication reviews and deprescribing as a single intervention in falls prevention: a systematic review and meta-analysis
- PMID: 36153749
- PMCID: PMC9509688
- DOI: 10.1093/ageing/afac191
Medication reviews and deprescribing as a single intervention in falls prevention: a systematic review and meta-analysis
Erratum in
-
Correction to: Guidelines for Falls in Older Adults, Medication reviews and deprescribing as a single intervention in falls prevention: a systematic review and meta-analysis, AND, World guidelines for falls prevention and management for older adults: a global initiative.Age Ageing. 2023 Sep 1;52(9):afad188. doi: 10.1093/ageing/afad188. Age Ageing. 2023. PMID: 37756648 Free PMC article. No abstract available.
Abstract
Background: our aim was to assess the effectiveness of medication review and deprescribing interventions as a single intervention in falls prevention.
Design: systematic review and meta-analysis.
Data sources: Medline, Embase, Cochrane CENTRAL, PsycINFO until 28 March 2022.
Eligibility criteria: randomised controlled trials of older participants comparing any medication review or deprescribing intervention with usual care and reporting falls as an outcome.
Study records: title/abstract and full-text screening by two reviewers.
Risk of bias: Cochrane Collaboration revised tool.
Data synthesis: results reported separately for different settings and sufficiently comparable studies meta-analysed.
Results: forty-nine heterogeneous studies were included.
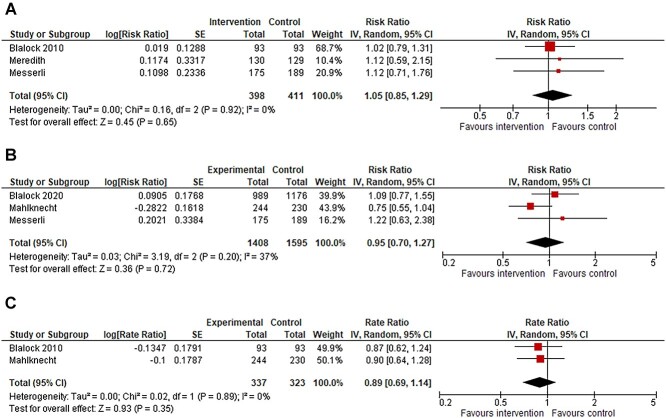
Community: meta-analyses of medication reviews resulted in a risk ratio (RR) of 1.05 (95% confidence interval, 0.85-1.29, I2 = 0%, 3 studies(s)) for number of fallers, in an RR = 0.95 (0.70-1.27, I2 = 37%, 3 s) for number of injurious fallers and in a rate ratio (RaR) of 0.89 (0.69-1.14, I2 = 0%, 2 s) for injurious falls.
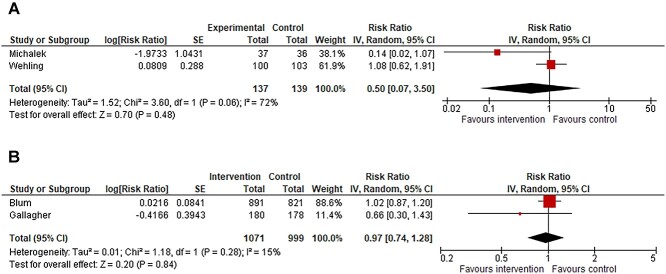
Hospital: meta-analyses assessing medication reviews resulted in an RR = 0.97 (0.74-1.28, I2 = 15%, 2 s) and in an RR = 0.50 (0.07-3.50, I2 = 72% %, 2 s) for number of fallers after and during admission, respectively.
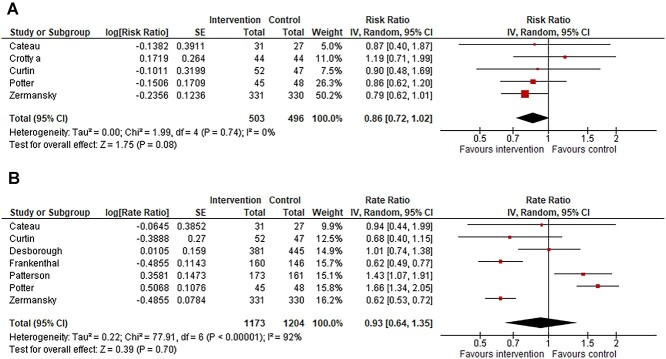
Long-term care: meta-analyses investigating medication reviews or deprescribing plans resulted in an RR = 0.86 (0.72-1.02, I2 = 0%, 5 s) for number of fallers and in an RaR = 0.93 (0.64-1.35, I2 = 92%, 7 s) for number of falls.
Conclusions: the heterogeneity of the interventions precluded us to estimate the exact effect of medication review and deprescribing as a single intervention. For future studies, more comparability is warranted. These interventions should not be implemented as a stand-alone strategy in falls prevention but included in multimodal strategies due to the multifactorial nature of falls.PROSPERO registration number: CRD42020218231.
Keywords: accidental falls; deprescribing; fall-risk-increasing drugs; medication review; older people; systematic review.
© The Author(s) 2022. Published by Oxford University Press on behalf of the British Geriatrics Society. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
None.
Figures