

How do predisposing factors differ between delirium motor subtypes? A systematic review and meta-analysis
- PMID: 36153750
- PMCID: PMC9509667
- DOI: 10.1093/ageing/afac200
How do predisposing factors differ between delirium motor subtypes? A systematic review and meta-analysis
Abstract
Background: Delirium is a common neurocognitive disorder in hospitalised older adults with vast negative consequences. The predominant method of subtyping delirium is by motor activity profile into hypoactive, hyperactive and mixed groups.
Objective: This systematic review and meta-analysis investigated how predisposing factors differ between delirium motor subtypes.
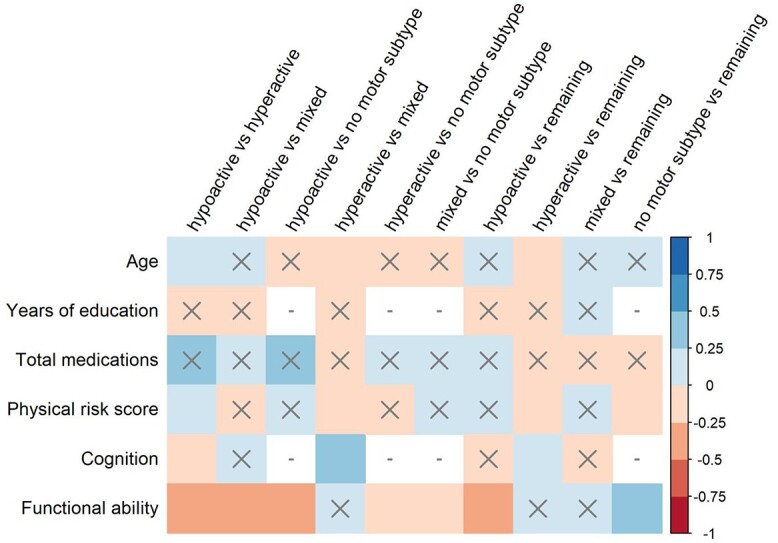
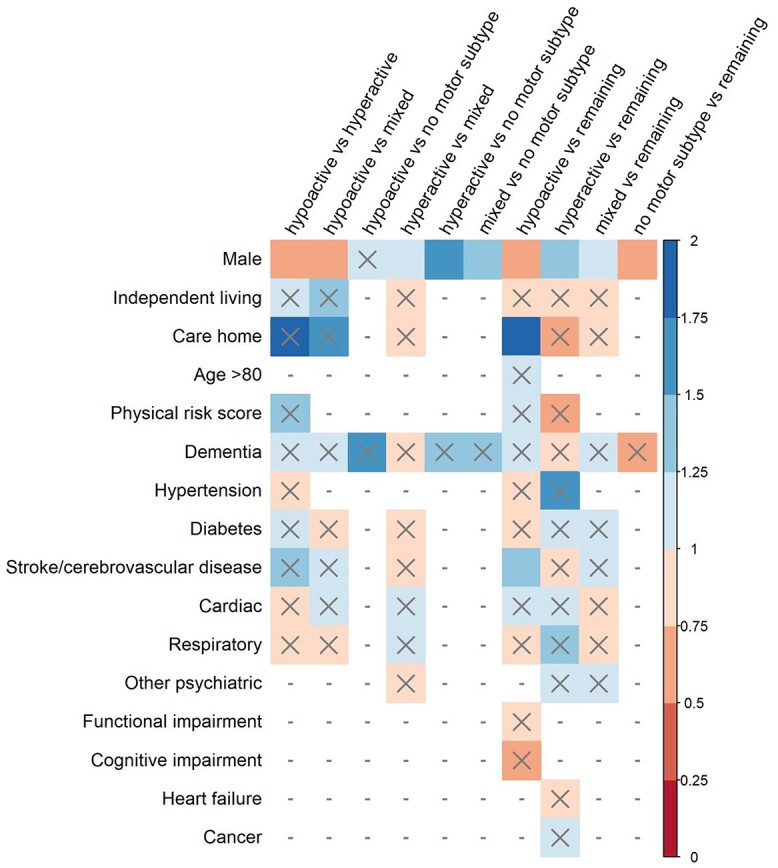
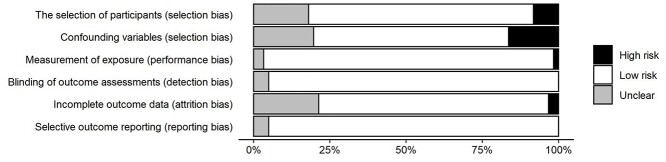
Methods: Databases (Medline, PsycINFO, Embase) were systematically searched for studies reporting predisposing factors (prior to delirium) for delirium motor subtypes. A total of 61 studies met inclusion criteria (N = 14,407, mean age 73.63 years). Random-effects meta-analyses synthesised differences between delirium motor subtypes relative to 22 factors.
Results: Hypoactive cases were older, had poorer cognition and higher physical risk scores than hyperactive cases and were more likely to be women, living in care homes, taking more medications, with worse functional performance and history of cerebrovascular disease than all remaining subtypes. Hyperactive cases were younger than hypoactive and mixed subtypes and were more likely to be men, with better cognition and lower physical risk scores than all other subtypes. Those with no motor subtype (unable to be classified) were more likely to be women and have better functional performance. Effect sizes were small.
Conclusions: Important differences in those who develop motor subtypes of delirium were shown prior to delirium occurrence. We provide robust quantitative evidence for a common clinical assumption that indices of frailty (institutional living, cognitive and functional impairment) are seen more in hypoactive patients. Motor subtypes should be measured across delirium research. Motor subtyping has great potential to improve the clinical risk assessment and management of delirium.
Keywords: hyperactive; hypoactive; mixed; older people; risk factor; systematic review.
© The Author(s) 2022. Published by Oxford University Press on behalf of the British Geriatrics Society. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Inouye SK, Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. Ann Intern Med 1990; 113: 941–8. - PubMed
-
- Robinson TN, Raeburn CD, Tran ZV, Angles EM, Brenner LA, Moss M. Postoperative delirium in the elderly: risk factors and outcomes. Ann Surg 2009; 249: 173–8. - PubMed
-
- Crocker E, Beggs T, Hassan Aet al. . Long-term effects of postoperative delirium in patients undergoing cardiac operation: a systematic review. Ann Thorac Surg 2016; 102: 1391–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
