

Comparison of acid-lowering drugs for endoscopy negative reflux disease: Systematic review and network Meta-Analysis
- PMID: 36153790
- PMCID: PMC10078414
- DOI: 10.1111/nmo.14469
Comparison of acid-lowering drugs for endoscopy negative reflux disease: Systematic review and network Meta-Analysis
Abstract
Background: The comparative efficacy and safety of medical therapies for gastro-esophageal reflux symptoms in endoscopy-negative reflux disease is unclear. We conducted a network meta-analysis to evaluate efficacy and safety of proton pump inhibitors (PPIs), histamine-2-receptor antagonists, potassium-competitive acid blockers (PCABs), and alginates in patients with endoscopy-negative reflux disease.
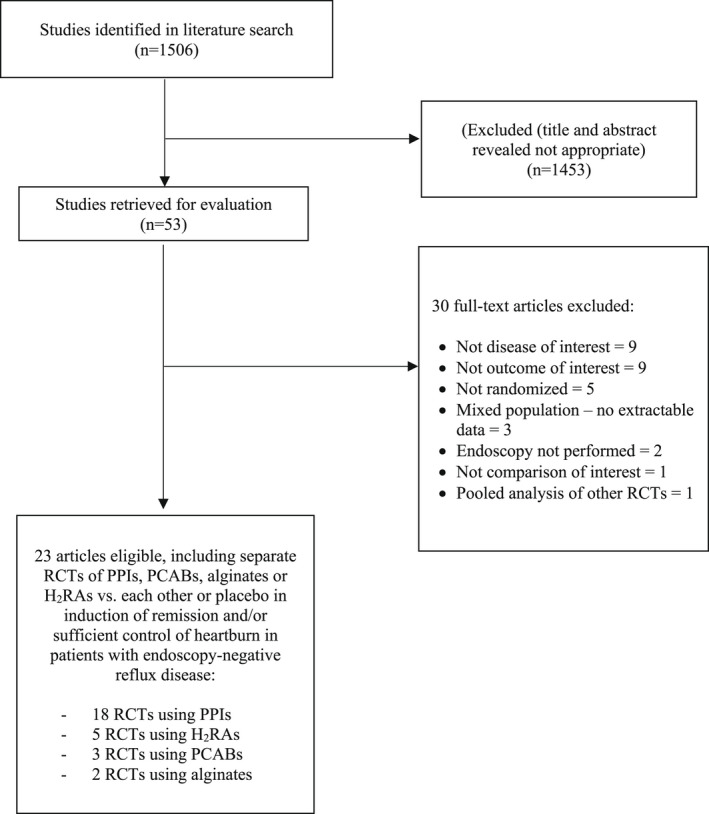
Methods: We searched MEDLINE, EMBASE, EMBASE Classic, and the Cochrane central register of controlled trials from inception to February 1, 2022. We included randomized controlled trials (RCTs) comparing efficacy of all drugs versus each other, or versus a placebo, in adults with endoscopy-negative reflux disease. Results were reported as pooled relative risks with 95% confidence intervals to summarize effect of each comparison tested, with treatments ranked according to P-score.
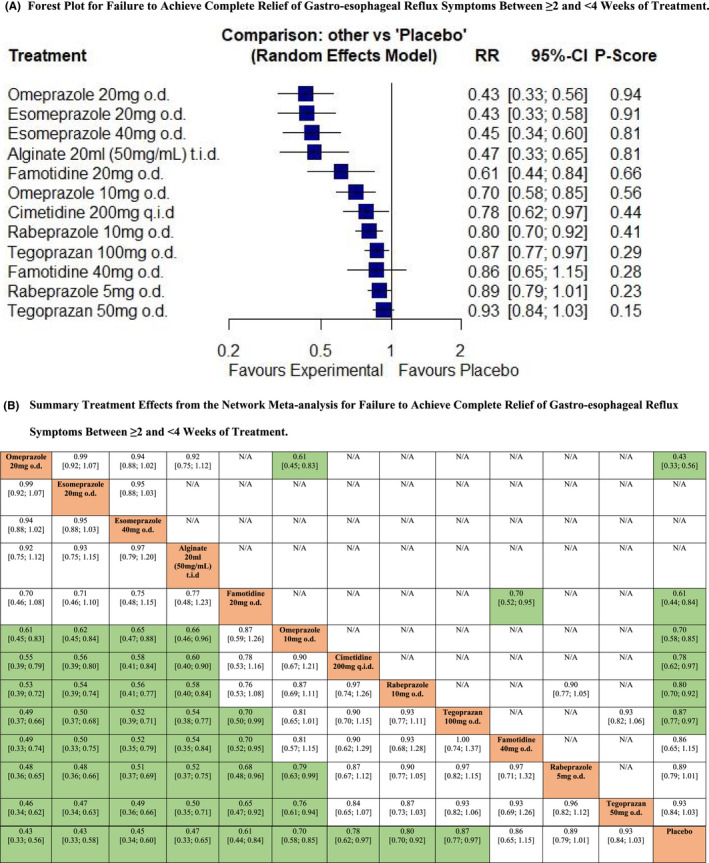
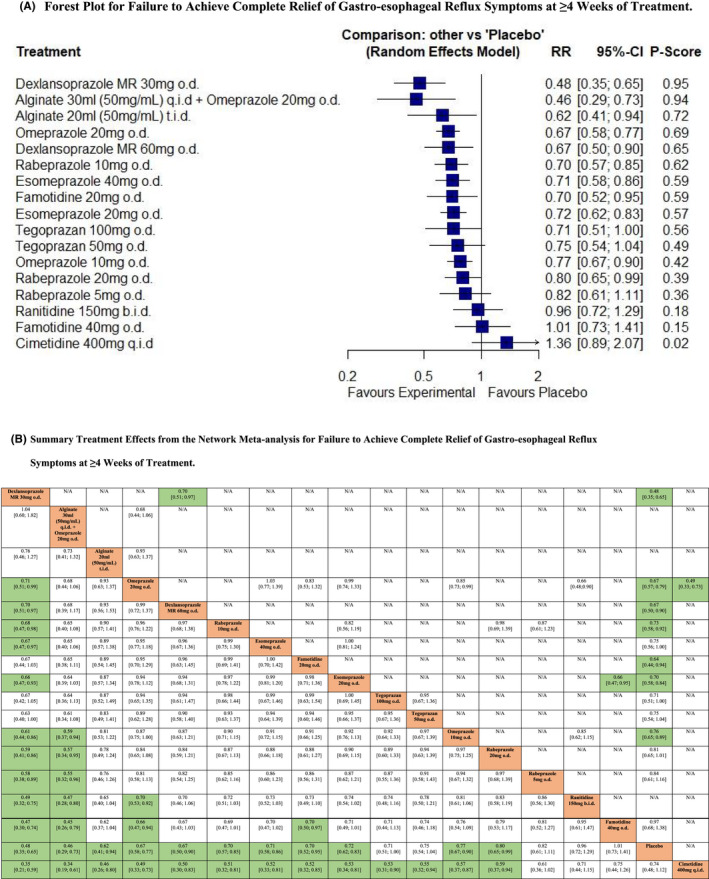
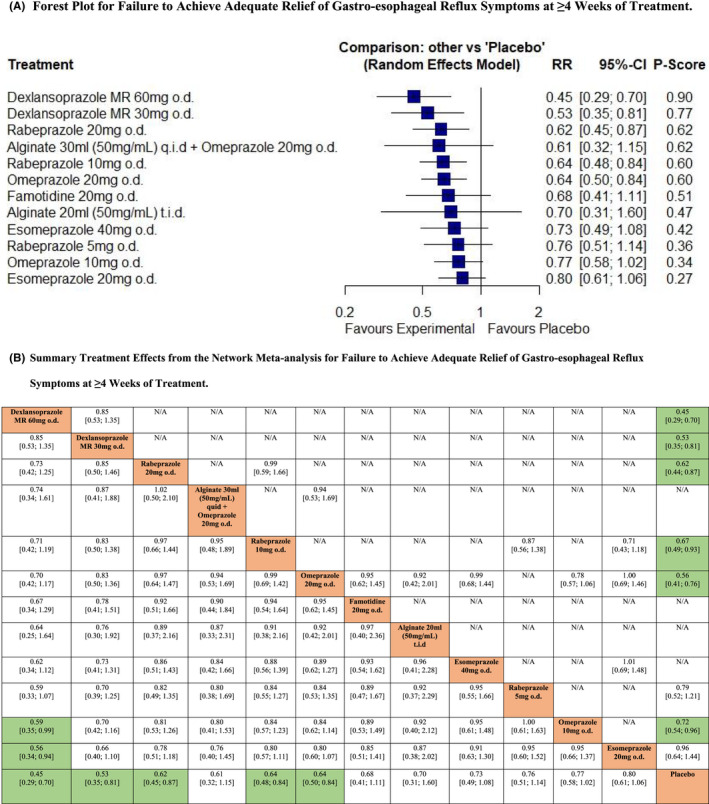
Key results: We identified 23 RCTs containing 10,735 subjects with endoscopy-negative reflux disease. Based on failure to achieve complete relief of symptoms between ≥2 and <4 weeks, omeprazole 20 mg o.d. (P-score 0.94) ranked first, with esomeprazole 20 mg o.d. or 40 mg o.d. ranked second and third. In achieving adequate relief, only rabeprazole 10 mg o.d. was significantly more efficacious than placebo. For failure to achieve complete relief at ≥4 weeks, dexlansoprazole 30 mg o.d. (P-score 0.95) ranked first, with 30 ml alginate q.i.d. combined with omeprazole 20 mg o.d., and 30 ml alginate t.i.d. second and third. In terms of failure to achieve adequate relief at ≥4 weeks, dexlansoprazole 60 mg o.d. ranked first (P-score 0.90), with dexlansoprazole 30 mg o.d. and rabeprazole 20 mg o.d. second and third. All drugs were safe and well-tolerated.
Conclusions & inferences: Our results confirm superiority of PPIs compared with most other drugs in treating endoscopy-negative reflux disease. Future RCTs should aim to better classify patients with endoscopy-negative reflux disease, and to establish the role of alginates and PCABs in achieving symptom relief in both the short- and long-term.
Keywords: alginate; endoscopy-negative reflux disease; histamine-2-receptor antagonist; potassium-competitive acid blocker; proton pump inhibitor.
© 2022 The Authors. Neurogastroenterology & Motility published by John Wiley & Sons Ltd.
Conflict of interest statement
Brigida Barberio: None. Pierfrancesco Visaggi: None. Edoardo V Savarino: None. Nicola de Bortoli: None. Christopher J. Black: None. Alexander C. Ford: None. Guarantor of the article: EVS is guarantor.
Figures

References
-
- Vakil N, Van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence‐based consensus. Am J Gastroenterol. 2006;101:1900‐1920. - PubMed
-
- Becher A, Dent J. Systematic review: ageing and gastro‐oesophageal reflux disease symptoms, oesophageal function and reflux oesophagitis. Aliment Pharmacol Ther. 2011;33:442‐454. - PubMed
-
- Hungin APS, Raghunath AS, Wiklund I. Beyond heartburn: a systematic review of the extra‐oesophageal spectrum of reflux‐induced disease. Fam Pract. 2005;22:591‐603. - PubMed
-
- Eusebi LH, Telese A, Cirota GG, et al. Systematic review with meta‐analysis: risk factors for Barrett's oesophagus in individuals with gastro‐oesophageal reflux symptoms. Aliment Pharmacol Ther. 2021;53:968‐976. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
