

Inadvertent QRS prolongation by an optimization device-based algorithm in patients with cardiac resynchronization therapy
- PMID: 36155997
- PMCID: PMC9512171
- DOI: 10.1371/journal.pone.0275276
Inadvertent QRS prolongation by an optimization device-based algorithm in patients with cardiac resynchronization therapy
Abstract
Background: Device-based algorithms offer the potential for automated optimization of cardiac resynchronization therapy (CRT), but the process for accepting them into clinical use is currently still ad-hoc, rather than based on pre-clinical and clinical testing of specific features of validity. We investigated how the QuickOpt-guided VV delay (VVD) programming performs against the clinical and engineering heuristic of QRS complex shortening by CRT.
Methods: A prospective, 2-center study enrolled 37 consecutive patients with CRT. QRS complex duration (QRSd) was assessed during intrinsic atrioventricular conduction, synchronous biventricular pacing, and biventricular pacing with QuickOpt-proposed VVD. The measurements were done manually by electronic calipers in signal-averaged and magnified 12-lead QRS complexes.
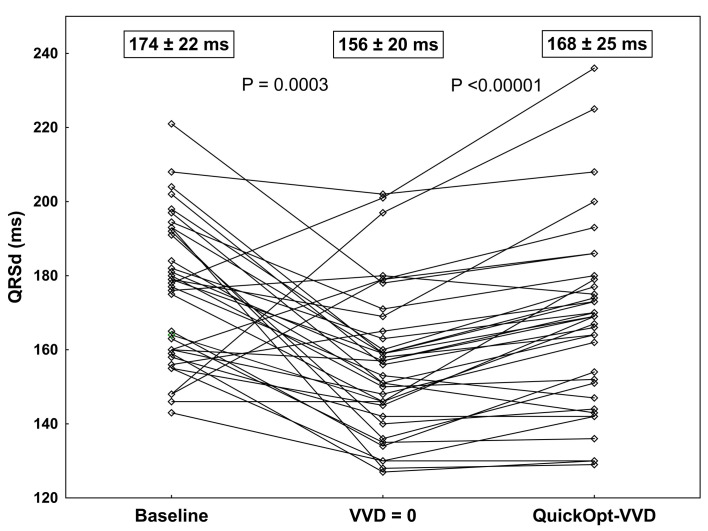
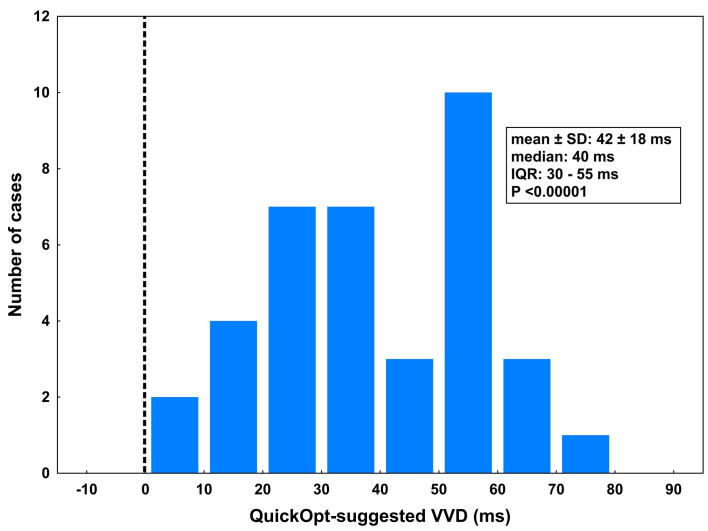
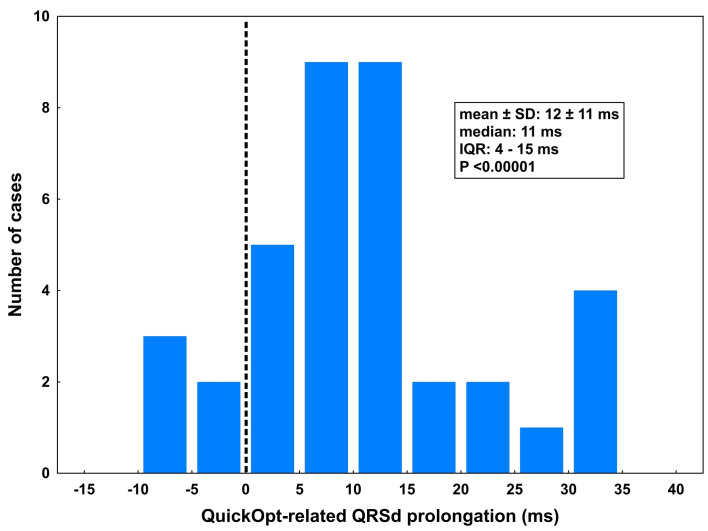
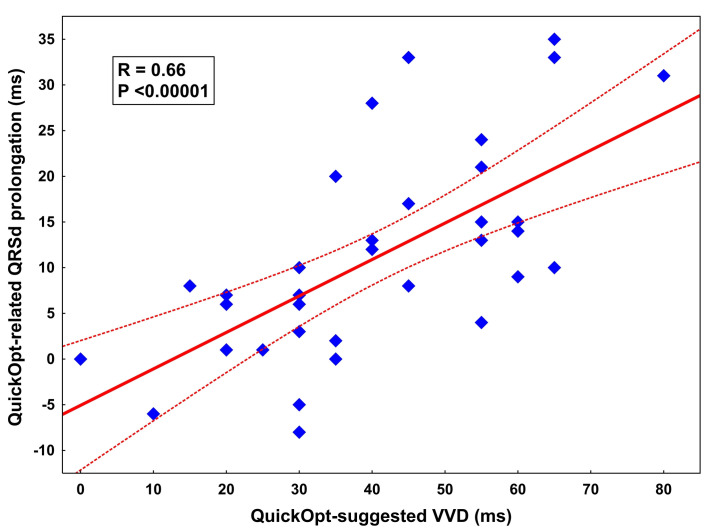
Results: Native QRSd was 174 ± 22 ms. Biventricular pacing with empiric AVD and synchronous VVD resulted in QRSd 156 ± 20 ms, a significant narrowing from the baseline QRSd by 17 ± 27 ms, P = 0.0003. In 36 of 37 patients, the QuickOpt algorithm recommended left ventricular preexcitation with VVD of 42 ± 18 ms (median 40 ms; interquartile range 30-55 ms, P <0.00001). QRSd in biventricular pacing with QuickOpt-based VVD was significantly longer compared with synchronous biventricular pacing (168 ± 25 ms vs. 156 ± 20 ms; difference 12 ± 11ms; P <0.00001). This prolongation correlated with the absolute VVD value (R = 0.66, P <0.00001).
Conclusions: QuickOpt algorithm systematically favours a left-preexcitation VVD which translates into a significant prolongation of the QRSd compared to synchronous biventricular pacing. There is no reason to believe that a manipulation that systematically widens QRSd should be considered to optimize physiology. Device-based CRT optimization algorithms should undergo systematic mechanistic pre-clinical evaluation in various scenarios before they are tested in large clinical studies.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Dr Kautzner reports personal fees from Bayer, Biosense Webster, Boehringer Ingelheim, Daiichi Sankyo, Medtronic, Merck Sharp & Dohme, Merit Medical, and St. Jude Medical (Abbott) for participation in scientific advisory boards, and has received speaker honoraria from Bayer, Biosense Webster, Biotronik, BMS, Boehringer Ingelheim, Daiichi Sankyo, Medtronic, Merck Sharp & Dohme, Mylan, Pfizer, ProMed, and St. Jude Medical (Abbott). All other authors declare no conflicts of interest regarding the paper. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Improvement of electrical synchrony in cardiac resynchronization therapy using dynamic atrioventricular delay programming and multipoint pacing.Pacing Clin Electrophysiol. 2021 Dec;44(12):1963-1971. doi: 10.1111/pace.14372. Epub 2021 Oct 21. Pacing Clin Electrophysiol. 2021. PMID: 34586643
-
Programming Cardiac Resynchronization Therapy for Electrical Synchrony: Reaching Beyond Left Bundle Branch Block and Left Ventricular Activation Delay.J Am Heart Assoc. 2018 Feb 6;7(3):e007489. doi: 10.1161/JAHA.117.007489. J Am Heart Assoc. 2018. PMID: 29432133 Free PMC article.
-
Dynamic programming of atrioventricular delay improves electrical synchrony in a multicenter cardiac resynchronization therapy study.Heart Rhythm. 2019 Jul;16(7):1047-1056. doi: 10.1016/j.hrthm.2019.01.020. Epub 2019 Jan 23. Heart Rhythm. 2019. PMID: 30682433
-
Electrocardiographic optimization techniques in resynchronization therapy.Europace. 2019 Sep 1;21(9):1286-1296. doi: 10.1093/europace/euz126. Europace. 2019. PMID: 31038177 Review.
-
Cardiac-resynchronization therapy in patients with systolic heart failure and QRS interval ≤130 ms: insights from a meta-analysis.Europace. 2015 Feb;17(2):267-73. doi: 10.1093/europace/euu214. Epub 2014 Aug 27. Europace. 2015. PMID: 25164431 Review.
References
-
- Sohaib SM, Kyriacou A, Jones S, Manisty CH, Mayet J, Kanagaratnam P, et al.. Evidence that conflict regarding size of haemodynamic response to interventricular delay optimization of cardiac resynchronization therapy may arise from differences in how atrioventricular delay is kept constant. Europace. 2015;17(12):1823–33. doi: 10.1093/europace/euu374 - DOI - PMC - PubMed
-
- Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, et al.. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013;34(29):2281–329. doi: 10.1093/eurheartj/eht150 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
