

Augmented renal clearance in the ICU: estimation, incidence, risk factors and consequences-a retrospective observational study
- PMID: 36156744
- PMCID: PMC9510087
- DOI: 10.1186/s13613-022-01058-w
Augmented renal clearance in the ICU: estimation, incidence, risk factors and consequences-a retrospective observational study
Abstract
Background: Augmented renal clearance (ARC) remains poorly evaluated in ICU. The objective of this study is to provide a full description of ARC in ICU including prevalence, evolution profile, risk factors and outcomes.
Methods: This was a retrospective, single-center, observational study. All the patients older than 18 years admitted for the first time in Medical ICU, Bichat, University Hospital, APHP, France, between January 1, 2017, and November 31, 2020 and included into the Outcomerea database with an ICU length of stay longer than 72 h were included. Patients with chronic kidney disease were excluded. Glomerular filtration rate was estimated each day during ICU stay using the measured creatinine renal clearance (CrCl). Augmented renal clearance (ARC) was defined as a 24 h CrCl greater than 130 ml/min/m2.
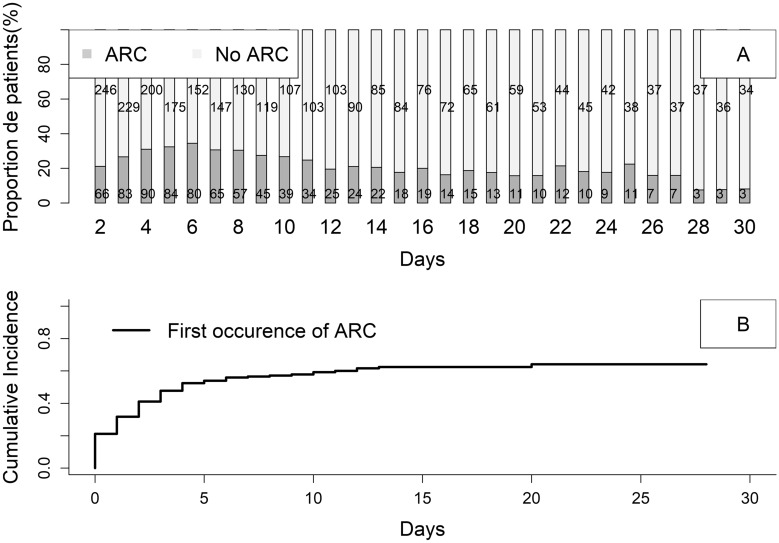
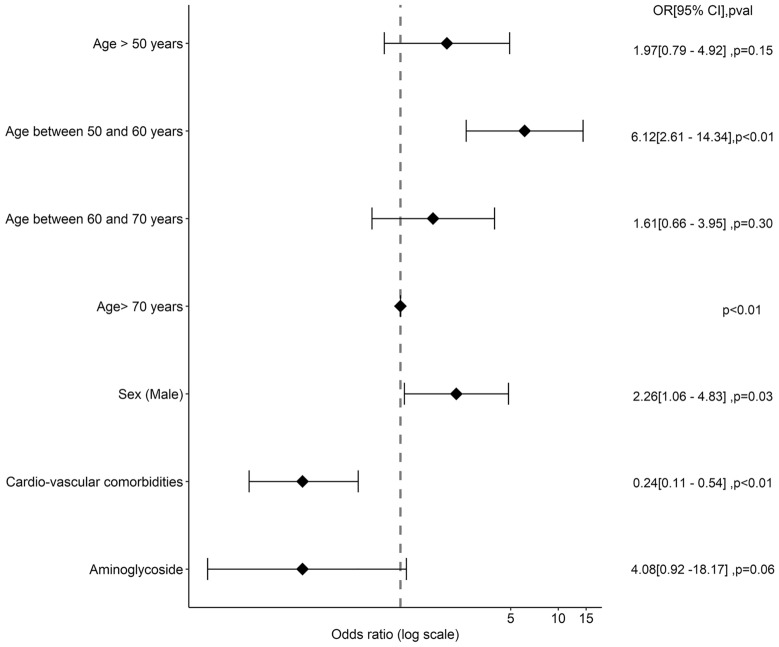
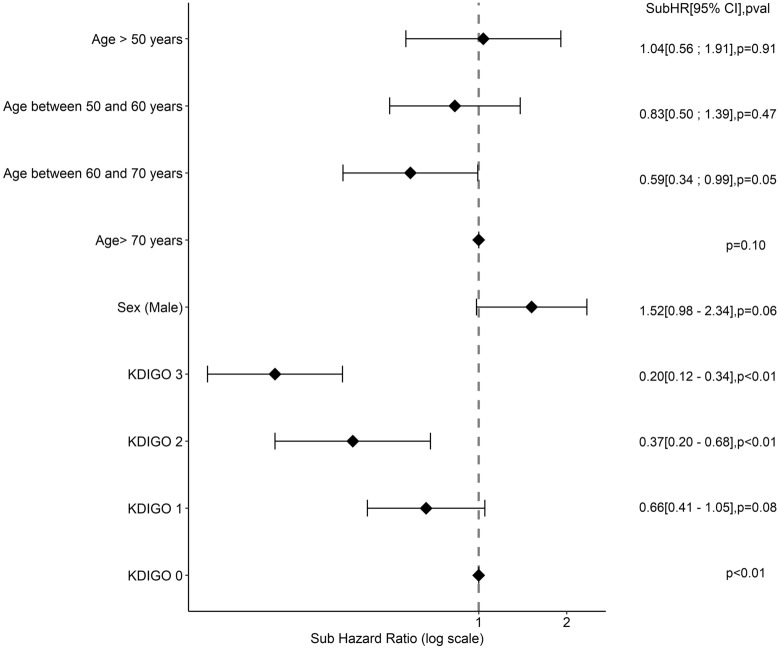
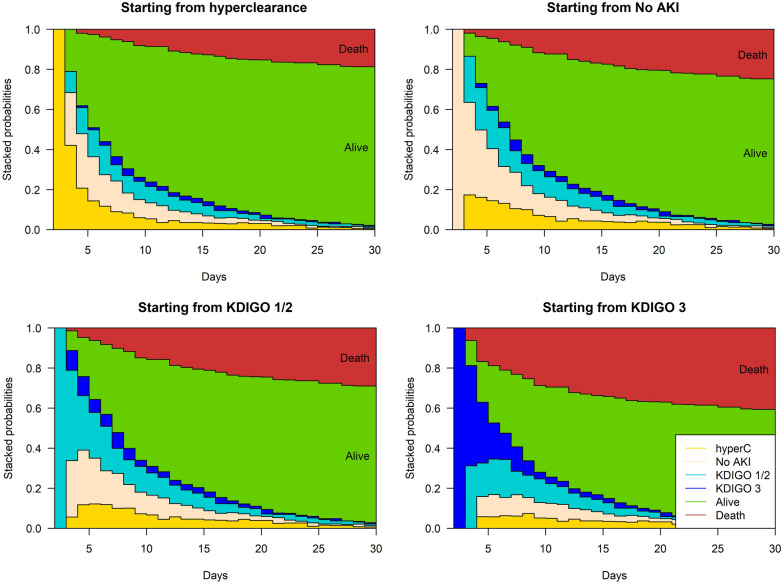
Results: 312 patients were included, with a median age of 62.7 years [51.4; 71.8], 106(31.9%) had chronic cardiovascular disease. The main reason for admission was acute respiratory failure (184(59%)) and 196(62.8%) patients had SARS-COV2. The median value for SAPS II score was 32[24; 42.5]; 146(44%) and 154(46.4%) patients were under vasopressors and invasive mechanical ventilation, respectively. The overall prevalence of ARC was 24.6% with a peak prevalence on Day 5 of ICU stay. The risk factors for the occurrence of ARC were young age and absence of cardiovascular comorbidities. The persistence of ARC during more than 10% of the time spent in ICU was significantly associated with a lower risk of death at Day 30.
Conclusion: ARC is a frequent phenomenon in the ICU with an increased incidence during the first week of ICU stay. Further studies are needed to assess its impact on patient prognosis.
Keywords: Augmented renal clearance; Epidemiology; Intensive care unit.
© 2022. The Author(s).
Conflict of interest statement
We declare that we have no conflicts of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous
