

Pathophysiology and Management of Pulmonary Embolism
- PMID: 36157092
- PMCID: PMC9507564
- DOI: 10.1055/s-0042-1756204
Pathophysiology and Management of Pulmonary Embolism
Abstract
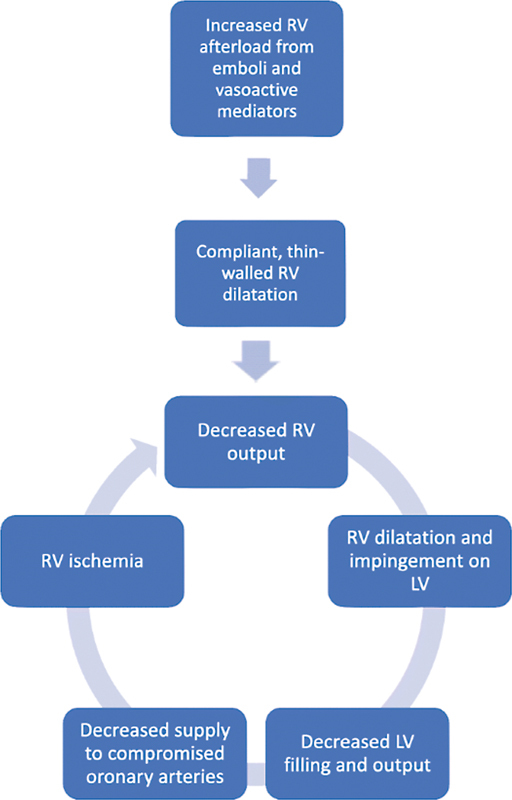
Pulmonary embolism (PE) is one of the most common etiologies of cardiovascular mortality. It could be linked to several risk factors including advanced age. The pathogenesis of PE is dictated by the Virchow's triad that includes venous stasis, endothelial injury, and a hypercoagulable state. The diagnosis of PE is difficult and is often missed due to the nonspecific symptomatology. Hypoxia is common in the setting of PE, and the degree of respiratory compromise is multifactorial and influenced by underlying cardiac function, clot location, and ability to compensate with respiratory mechanics. Right ventricular dysfunction/failure is the more profound cardiovascular impact of acute PE and occurs due to sudden increase in afterload. This is also the primary cause of death in PE. High clinical suspicion is required in those with risk factors and presenting signs or symptoms of venous thromboembolic disease, with validated clinical risk scores such as the Wells, Geneva, and pulmonary embolism rule out criteria in estimating the likelihood for PE. Advancement in capture time and wider availability of computed tomographic pulmonary angiography and D-dimer testing have further facilitated the rapid evaluation and diagnosis of suspected PE. Treatment is dependent on clinical presentation and initially involves providing adequate oxygenation and stabilizing hemodynamics. Anticoagulant therapy is indicated for the treatment of PE. Treatment is guided by presence or absence of shock and ranges from therapeutic anticoagulation to pharmacologic versus mechanical thrombectomy. The prognosis of patients can vary considerably depending on the cardiac and pulmonary status of patient and the size of the embolus.
Keywords: Virchow's triad; deep venous thrombosis; hypoxia; pulmonary angiography; pulmonary embolism; pulmonary hypertension; thromboembolic disease.
International College of Angiology. This article is published by Thieme.
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
Acute Pulmonary Embolism: Contemporary Approach to Diagnosis, Risk-Stratification, and Management.Int J Angiol. 2019 Jun;28(2):100-111. doi: 10.1055/s-0039-1692636. Epub 2019 Jul 5. Int J Angiol. 2019. PMID: 31384107 Free PMC article.
-
[Pulmonary thromboembolism: incidence, physiopathology, diagnosis and treatment].Tunis Med. 2014 Jul;92(7):435-47. Tunis Med. 2014. PMID: 25775281 Review. French.
-
Retrospective validation of the pulmonary embolism rule-out criteria rule in 'PE unlikely' patients with suspected pulmonary embolism.Eur J Emerg Med. 2018 Jun;25(3):185-190. doi: 10.1097/MEJ.0000000000000442. Eur J Emerg Med. 2018. PMID: 28002070
-
Clinical prediction of pulmonary embolism in respiratory emergencies.Thromb Res. 2011 May;127(5):411-7. doi: 10.1016/j.thromres.2011.02.002. Epub 2011 Mar 10. Thromb Res. 2011. PMID: 21396683
-
Managing pulmonary embolism from presentation to extended treatment.Thromb Res. 2014 Feb;133(2):139-48. doi: 10.1016/j.thromres.2013.09.040. Epub 2013 Oct 14. Thromb Res. 2014. PMID: 24182642 Review.
Cited by
-
Pulmonary Embolism in Donor Lungs-Incidence and Management.Int J Angiol. 2024 Mar 15;33(2):128-131. doi: 10.1055/s-0044-1782536. eCollection 2024 Jun. Int J Angiol. 2024. PMID: 38846992 Free PMC article. Review.
-
Exploring varied radiologic appearance in pulmonary embolism with CT pulmonary angiography: Case series with literature review.Radiol Case Rep. 2024 May 23;19(8):3367-3371. doi: 10.1016/j.radcr.2024.04.081. eCollection 2024 Aug. Radiol Case Rep. 2024. PMID: 38827043 Free PMC article.
-
Venous Thromboembolism: Current Insights and Future Directions.Int J Angiol. 2024 Jul 8;33(4):250-261. doi: 10.1055/s-0044-1787652. eCollection 2024 Dec. Int J Angiol. 2024. PMID: 39502354 Free PMC article. Review.
-
Diagnostic Strategies in Pulmonary Embolism.Int J Angiol. 2024 Feb 12;33(2):89-94. doi: 10.1055/s-0044-1779661. eCollection 2024 Jun. Int J Angiol. 2024. PMID: 38846998 Free PMC article. Review.
-
Prevalence and clinical burden of venous thromboembolic events (VTEs) in contemporary total knee arthroplasties (TKAs) in US hospitals.J Orthop. 2024 Oct 8;61:122-126. doi: 10.1016/j.jor.2024.10.006. eCollection 2025 Mar. J Orthop. 2024. PMID: 40051786
References
-
- ISTH Steering Committee for World Thrombosis Day . Raskob G E, Angchaisuksiri P, Blanco A N. Thrombosis: a major contributor to global disease burden. Semin Thromb Hemost. 2014;40(07):724–735. - PubMed
-
- Anderson F A, Jr, Zayaruzny M, Heit J A, Fidan D, Cohen A T. Estimated annual numbers of US acute-care hospital patients at risk for venous thromboembolism. Am J Hematol. 2007;82(09):777–782. - PubMed
-
- Silverstein M D, Heit J A, Mohr D N, Petterson T M, O'Fallon W M, Melton L J., III Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998;158(06):585–593. - PubMed
-
- Dudzinski D M, Giri J, Rosenfield K. Interventional treatment of pulmonary embolism. Circ Cardiovasc Interv. 2017;10(02):e004345. - PubMed
-
- Huet Y, Lemaire F, Brun-Buisson C. Hypoxemia in acute pulmonary embolism. Chest. 1985;88(06):829–836. - PubMed