

Current Management of Heart Failure with Preserved Ejection Fraction
- PMID: 36157094
- PMCID: PMC9507602
- DOI: 10.1055/s-0042-1756173
Current Management of Heart Failure with Preserved Ejection Fraction
Abstract
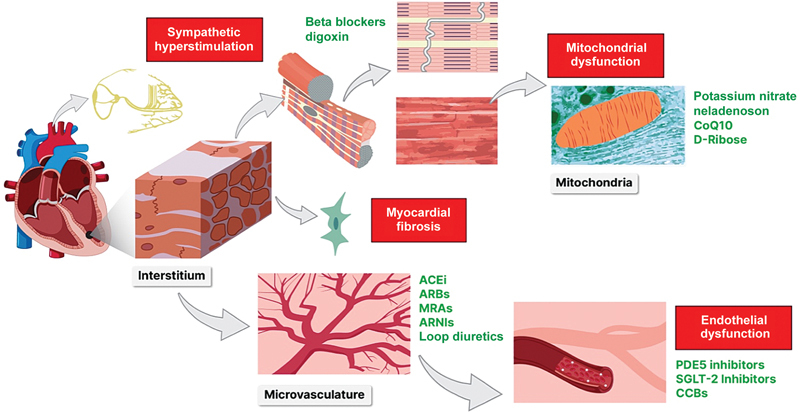
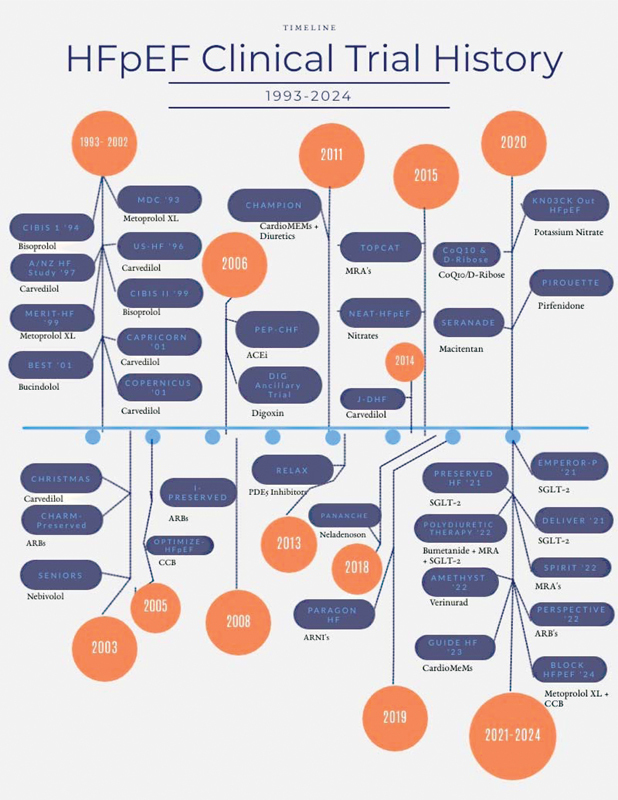
Heart failure with preserved ejection fraction (HFpEF) encompasses nearly half of heart failure (HF) worldwide, and still remains a poor prognostic indicator. It commonly coexists in patients with vascular disease and needs to be recognized and managed appropriately to reduce morbidity and mortality. Due to the heterogeneity of HFpEF as a disease process, targeted pharmacotherapy to this date has not shown a survival benefit among this population. This article serves as a comprehensive historical review focusing on the management of HFpEF by reviewing past, present, and future randomized controlled trials that attempt to uncover a therapeutic value. With a paradigm shift in the pathophysiology of HFpEF as an inflammatory, neurohormonal, and interstitial process, a phenotypic approach has increased in popularity focusing on the treatment of HFpEF as a systemic disease. This article also addresses common comorbidities associated with HFpEF as well as current and ongoing clinical trials looking to further elucidate such links.
Keywords: BNP; HFpEF; diastolic dysfunction; heart failure; pathophysiology; preserved ejection fraction; treatment of HFpEF.
International College of Angiology. This article is published by Thieme.
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation.J Am Coll Cardiol. 2013 Jul 23;62(4):263-71. doi: 10.1016/j.jacc.2013.02.092. Epub 2013 May 15. J Am Coll Cardiol. 2013. PMID: 23684677 Review.
-
Drug Targets for Heart Failure with Preserved Ejection Fraction: A Mechanistic Approach and Review of Contemporary Clinical Trials.Annu Rev Pharmacol Toxicol. 2019 Jan 6;59:41-63. doi: 10.1146/annurev-pharmtox-010818-021136. Epub 2018 Oct 8. Annu Rev Pharmacol Toxicol. 2019. PMID: 30296895 Free PMC article. Review.
-
Understanding heart failure with preserved ejection fraction: where are we today?Neth Heart J. 2016 Apr;24(4):227-36. doi: 10.1007/s12471-016-0810-1. Neth Heart J. 2016. PMID: 26909795 Free PMC article. Review.
-
Clinical Phenotypes of Heart Failure With Preserved Ejection Fraction to Select Preclinical Animal Models.JACC Basic Transl Sci. 2022 May 25;7(8):844-857. doi: 10.1016/j.jacbts.2021.12.009. eCollection 2022 Aug. JACC Basic Transl Sci. 2022. PMID: 36061340 Free PMC article. Review.
-
Drugs That Ameliorate Epicardial Adipose Tissue Inflammation May Have Discordant Effects in Heart Failure With a Preserved Ejection Fraction as Compared With a Reduced Ejection Fraction.J Card Fail. 2019 Dec;25(12):986-1003. doi: 10.1016/j.cardfail.2019.09.002. Epub 2019 Sep 18. J Card Fail. 2019. PMID: 31541742 Review.
Cited by
-
Risk factors for prolonged hospitalization in acute decompensated heart failure from the HEROES study.Sci Rep. 2025 Aug 9;15(1):29133. doi: 10.1038/s41598-025-14100-1. Sci Rep. 2025. PMID: 40783608 Free PMC article.
References
-
- McKee P A, Castelli W P, McNamara P M, Kannel W B. The natural history of congestive heart failure: the Framingham study. N Engl J Med. 1971;285(26):1441–1446. - PubMed
-
- Butrous H, Pai R G. Heart failure with normal ejection fraction: current diagnostic and management strategies. Expert Rev Cardiovasc Ther. 2013;11(09):1179–1193. - PubMed
-
- Bleumink G S, Knetsch A M, Sturkenboom M C. Quantifying the heart failure epidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure The Rotterdam Study. Eur Heart J. 2004;25(18):1614–1619. - PubMed
-
- Framingham Heart Study . Lloyd-Jones D M, Larson M G, Leip E P. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation. 2002;106(24):3068–3072. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
