

Current trends in regenerative liver surgery: Novel clinical strategies and experimental approaches
- PMID: 36157407
- PMCID: PMC9491020
- DOI: 10.3389/fsurg.2022.903825
Current trends in regenerative liver surgery: Novel clinical strategies and experimental approaches
Abstract
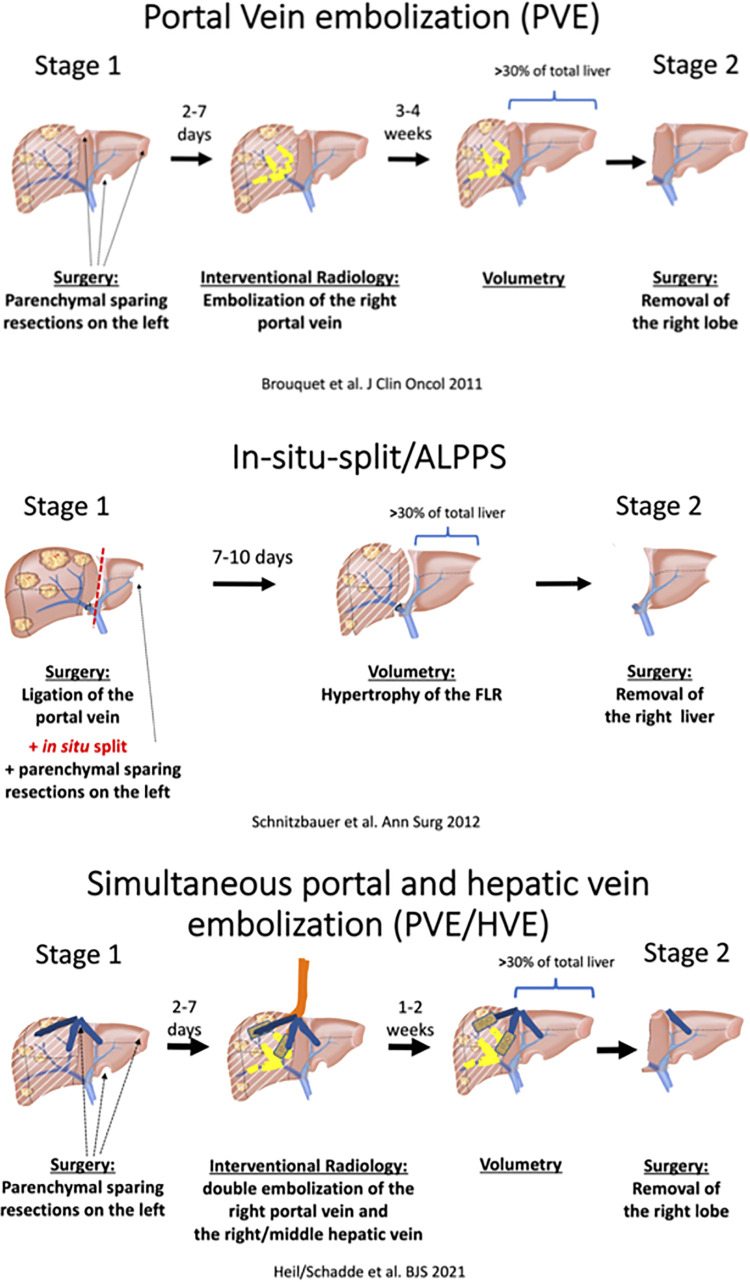
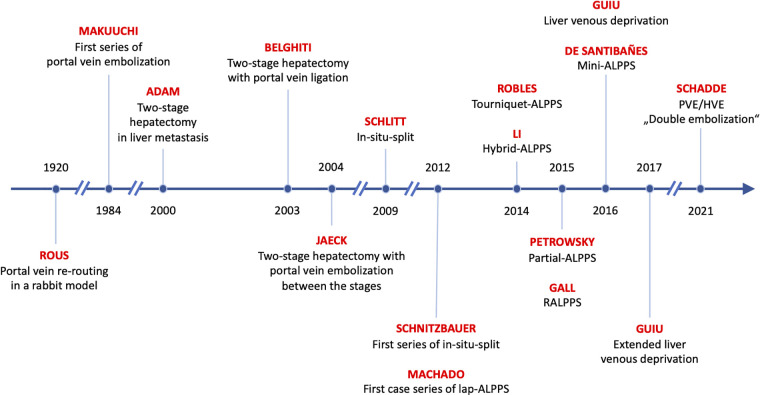
Liver resections are performed to cure patients with hepatobiliary malignancies and metastases to the liver. However, only a small proportion of patients is resectable, largely because only up to 70% of liver tissue is expendable in a resection. If larger resections are performed, there is a risk of post-hepatectomy liver failure. Regenerative liver surgery addresses this limitation by increasing the future liver remnant to an appropriate size before resection. Since the 1980s, this surgery has evolved from portal vein embolization (PVE) to a multiplicity of methods. This review presents an overview of the available methods and their advantages and disadvantages. The first use of PVE was in patients with large hepatocellular carcinomas. The increase in liver volume induced by PVE equals that of portal vein ligation, but both result only in a moderate volume increase. While awaiting sufficient liver growth, 20%-40% of patients fail to achieve resection, mostly due to the progression of disease. The MD Anderson Cancer Centre group improved the PVE methodology by adding segment 4 embolization ("high-quality PVE") and demonstrated that oncological results were better than non-surgical approaches in this previously unresectable patient population. In 2012, a novel method of liver regeneration was proposed and called Associating Liver Partition and Portal vein ligation for Staged hepatectomy (ALPPS). ALPPS accelerated liver regeneration by a factor of 2-3 and increased the resection rate to 95%-100%. However, ALPPS fell short of expectations due to a high mortality rate and a limited utility only in highly selected patients. Accelerated liver regeneration, however, was there to stay. This is evident in the multiplicity of ALPPS modifications like radiofrequency or partial ALPPS. Overall, rapid liver regeneration allowed an expansion of resectability with increased perioperative risk. But, a standardized low-risk approach to rapid hypertrophy has been missing and the techniques used and in use depend on local expertise and preference. Recently, however, simultaneous portal and hepatic vein embolization (PVE/HVE) appears to offer both rapid hypertrophy and no increased clinical risk. While prospective randomized comparisons are underway, PVE/HVE has the potential to become the future gold standard.
Keywords: ALPPS; future liver remnant; liver venous deprivation; portal vein embolization; regenerative liver surgery; resectability; simultaneous portal and hepatic vein embolization.
© 2022 Heil, Schiesser and Schadde.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources