

Melanoma: Molecular genetics, metastasis, targeted therapies, immunotherapies, and therapeutic resistance
- PMID: 36157497
- PMCID: PMC9485270
- DOI: 10.1016/j.gendis.2022.04.004
Melanoma: Molecular genetics, metastasis, targeted therapies, immunotherapies, and therapeutic resistance
Abstract
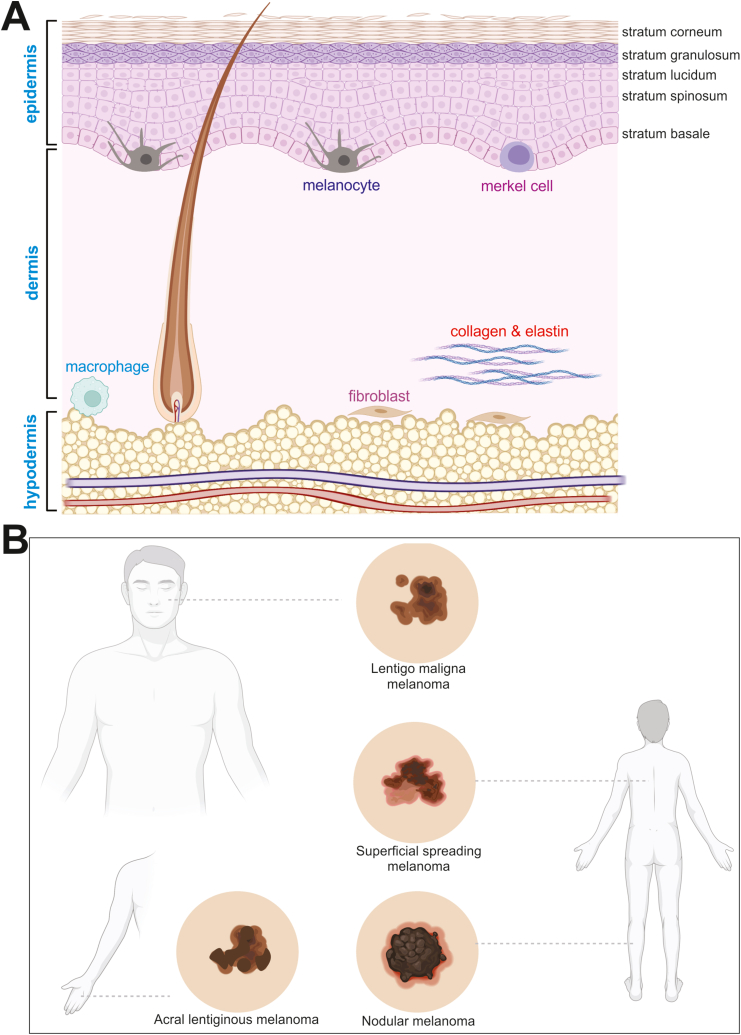
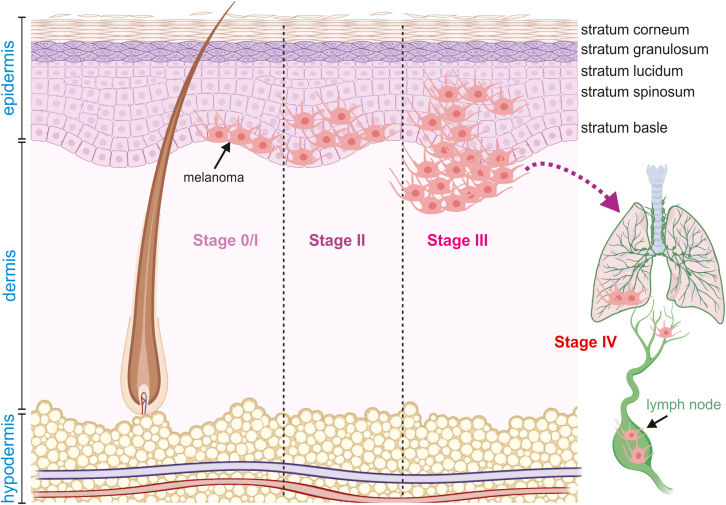
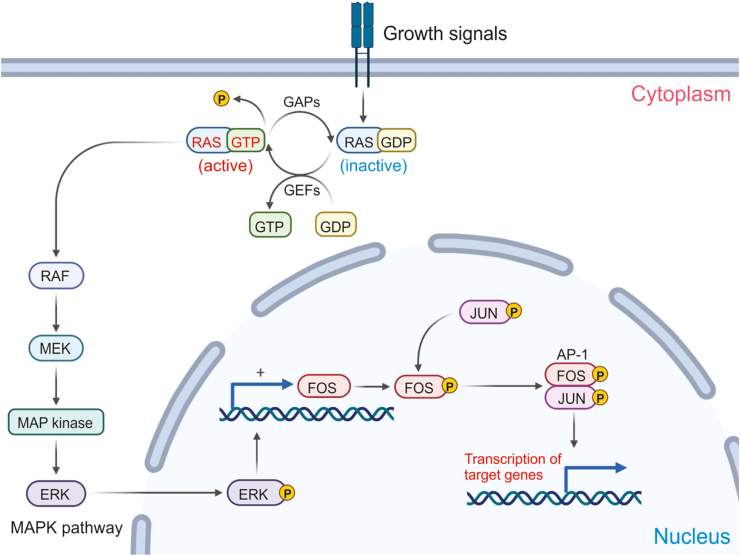
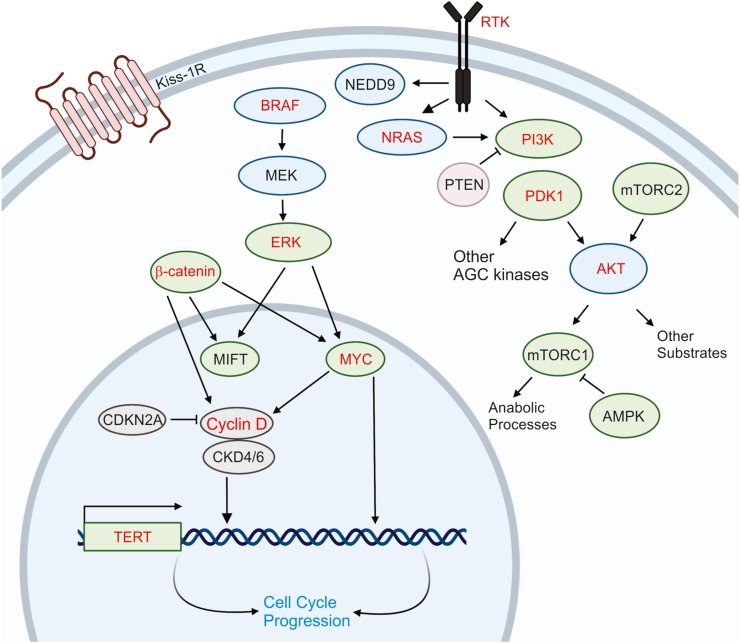
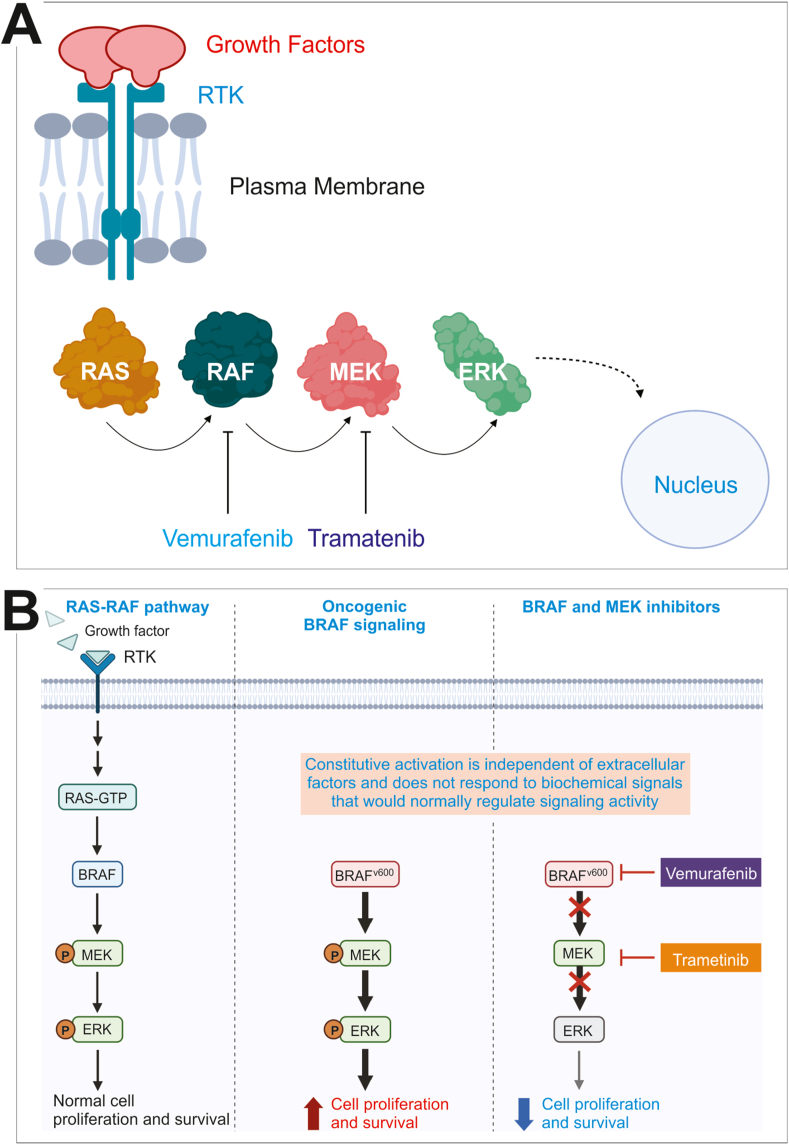
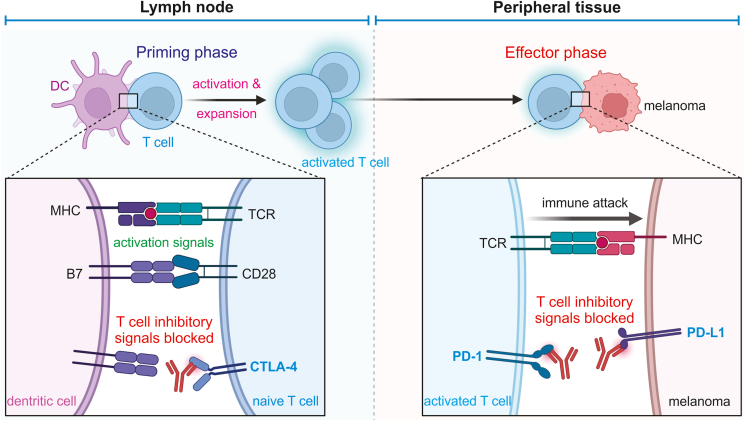
Cutaneous melanoma is a common cancer and cases have steadily increased since the mid 70s. For some patients, early diagnosis and surgical removal of melanomas is lifesaving, while other patients typically turn to molecular targeted therapies and immunotherapies as treatment options. Easy sampling of melanomas allows the scientific community to identify the most prevalent mutations that initiate melanoma such as the BRAF, NRAS, and TERT genes, some of which can be therapeutically targeted. Though initially effective, many tumors acquire resistance to the targeted therapies demonstrating the need to investigate compensatory pathways. Immunotherapies represent an alternative to molecular targeted therapies. However, inter-tumoral immune cell populations dictate initial therapeutic response and even tumors that responded to treatment develop resistance in the long term. As the protocol for combination therapies develop, so will our scientific understanding of the many pathways at play in the progression of melanoma. The future direction of the field may be to find a molecule that connects all of the pathways. Meanwhile, noncoding RNAs have been shown to play important roles in melanoma development and progression. Studying noncoding RNAs may help us to understand how resistance - both primary and acquired - develops; ultimately allow us to harness the true potential of current therapies. This review will cover the basic structure of the skin, the mutations and pathways responsible for transforming melanocytes into melanomas, the process by which melanomas metastasize, targeted therapeutics, and the potential that noncoding RNAs have as a prognostic and treatment tool.
Keywords: BRAF inhibitors; Checkpoint inhibitors; Drug resistance; Immunotherapy; Melanoma; Melanoma metastasis; Skin cancer; Targeted therapy; Therapeutic resistance.
© 2022 Chongqing Medical University. Production and hosting by Elsevier B.V.
Figures
References
-
- Miller A.J., Mihm M.C., Jr. Melanoma. N Engl J Med. 2006;355(1):51–65. - PubMed
-
- Eggermont A.M., Spatz A., Robert C. Cutaneous melanoma. Lancet. 2014;383(9919):816–827. - PubMed
-
- Kanitakis J. Anatomy, histology and immunohistochemistry of normal human skin. Eur J Dermatol. 2002;12(4):390–399. - PubMed
-
- Kolarsick P., Kolarsick M., Goodwin C. Anatomy and physiology of the skin. J Dermatol Nurses Assoc. 2011;3(4):203–213.
-
- Freedberg I., Eisen A., Wolff K., Austen K., Goldsmith L., Katz S. 6th ed. McGraw-Hill Education; 2003. Fitzpatrick's Dermatology in General Medicine.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
