

Retinoblastoma in an older child with secondary glaucoma as the first clinical presenting symptom: A case report
- PMID: 36157816
- PMCID: PMC9453347
- DOI: 10.12998/wjcc.v10.i24.8695
Retinoblastoma in an older child with secondary glaucoma as the first clinical presenting symptom: A case report
Abstract
Background: Retinoblastoma (Rb) is primarily found in infants or young children. The most common primary presenting sign of Rb is leukocoria. Rb is very rare in children who are 10 years old or older. Timely and correct diagnosis as well as proper treatment are the key factors affecting the prognosis of Rb.
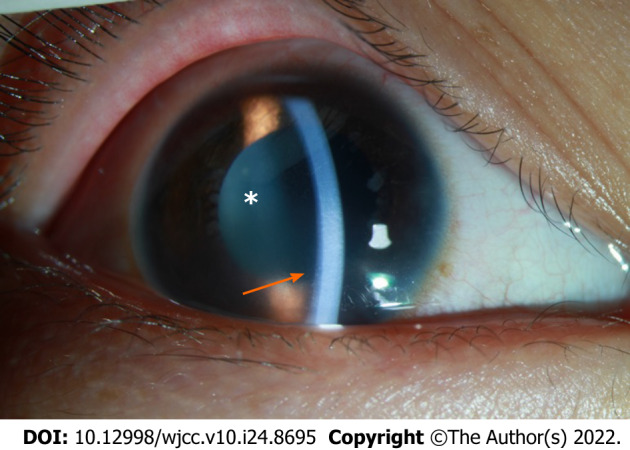
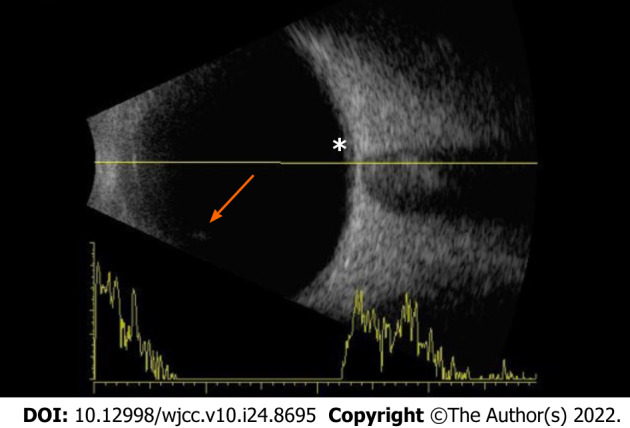
Case summary: A 10-year-old girl with symptoms of vision loss, redness, swelling and pain in the right eye for 2 mo was admitted to our Department of Ophthalmology. The visual acuity of the right eye was graded as hand movement. The intraocular pressure of the eye was 46.9 mmHg. No substantial space-occupying lesion or characteristic calcified plaque was found in the eye. The patient underwent anterior chamber irrigation under general anesthesia on the same day of admission, and 2 mL of irrigation solution was saved for pathological examination. Histopathological examination of the anterior chamber fluid revealed cancer cells. A diagnosis of Rb with masquerade syndrome was made. The patient underwent enucleation followed by 6 rounds of systematic chemotherapy. A follow-up examination almost 9 years later found no relapse of Rb.
Conclusion: For older pediatric patients who have secondary glaucoma and uveitis symptoms without a clear cause of the disease and have no space-occupying lesion found by imaging examination, aqueous humor or vitreous humor examination is recommended for timely and correct diagnosis and appropriate treatment.
Keywords: Case report; Masquerade syndrome; Older children; Retinoblastoma; Secondary glaucoma; Uveitis.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflicts of interest.
Figures






References
-
- AlAli A, Kletke S, Gallie B, Lam WC. Retinoblastoma for Pediatric Ophthalmologists. Asia Pac J Ophthalmol (Phila) 2018;7:160–168. - PubMed
-
- Broaddus E, Topham A, Singh AD. Incidence of retinoblastoma in the USA: 1975-2004. Br J Ophthalmol. 2009;93:21–23. - PubMed
-
- Dimaras H, Kimani K, Dimba EA, Gronsdahl P, White A, Chan HS, Gallie BL. Retinoblastoma. Lancet. 2012;379:1436–1446. - PubMed
-
- Fabian ID, Onadim Z, Karaa E, Duncan C, Chowdhury T, Scheimberg I, Ohnuma SI, Reddy MA, Sagoo MS. The management of retinoblastoma. Oncogene. 2018;37:1551–1560. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
