

Personalizing treatment in end-stage kidney disease: deciding between haemodiafiltration and haemodialysis based on individualized treatment effect prediction
- PMID: 36158156
- PMCID: PMC9494541
- DOI: 10.1093/ckj/sfac153
Personalizing treatment in end-stage kidney disease: deciding between haemodiafiltration and haemodialysis based on individualized treatment effect prediction
Abstract
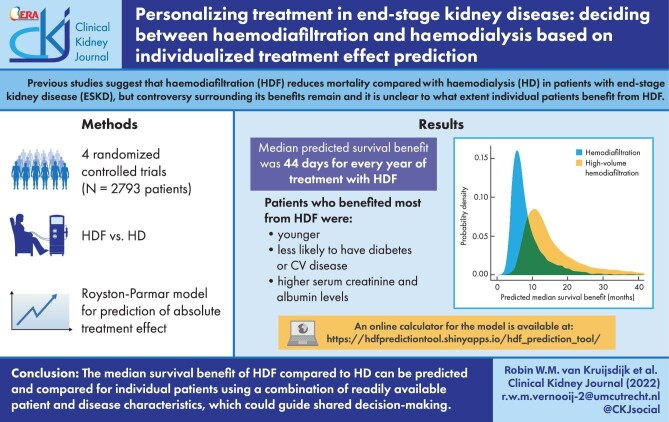
Background: Previous studies suggest that haemodiafiltration reduces mortality compared with haemodialysis in patients with end-stage kidney disease (ESKD), but the controversy surrounding its benefits remains and it is unclear to what extent individual patients benefit from haemodiafiltration. This study is aimed to develop and validate a treatment effect prediction model to determine which patients would benefit most from haemodiafiltration compared with haemodialysis in terms of all-cause mortality.
Methods: Individual participant data from four randomized controlled trials comparing haemodiafiltration with haemodialysis on mortality were used to derive a Royston-Parmar model for the prediction of absolute treatment effect of haemodiafiltration based on pre-specified patient and disease characteristics. Validation of the model was performed using internal-external cross validation.
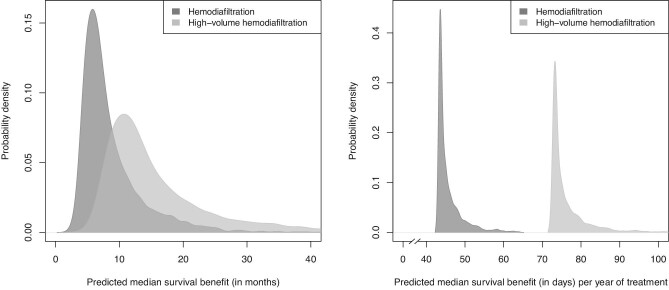
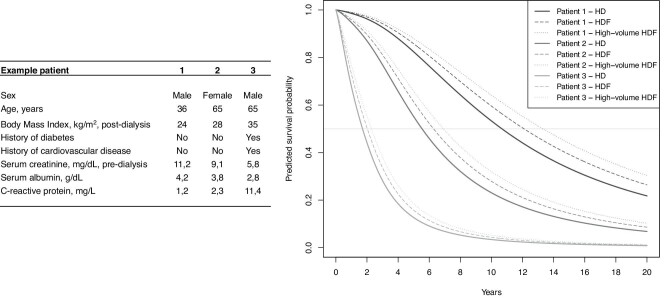
Results: The median predicted survival benefit was 44 (Q1-Q3: 44-46) days for every year of treatment with haemodiafiltration compared with haemodialysis. The median survival benefit with haemodiafiltration ranged from 2 to 48 months. Patients who benefitted most from haemodiafiltration were younger, less likely to have diabetes or a cardiovascular history and had higher serum creatinine and albumin levels. Internal-external cross validation showed adequate discrimination and calibration.
Conclusion: Although overall mortality is reduced by haemodiafiltration compared with haemodialysis in ESKD patients, the absolute survival benefit can vary greatly between individuals. Our results indicate that the effects of haemodiafiltration on survival can be predicted using a combination of readily available patient and disease characteristics, which could guide shared decision-making.
Keywords: haemodiafiltration; haemodialysis; treatment effect heterogeneity; treatment effect prediction.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures
References
-
- Liyanage T, Ninomiya T, Jha Vet al. . Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet North Am Ed 2015; 385: 1975–1982 - PubMed
-
- Tattersall JE, Ward RA.. Online haemodiafiltration: definition, dose quantification and safety revisited. Nephrol Dial Transplant 2013; 28: 542–550 - PubMed
LinkOut - more resources
Full Text Sources
