

Novel index for the prediction of significant liver fibrosis and cirrhosis in chronic hepatitis B patients in China
- PMID: 36158257
- PMCID: PMC9346453
- DOI: 10.3748/wjg.v28.i27.3503
Novel index for the prediction of significant liver fibrosis and cirrhosis in chronic hepatitis B patients in China
Abstract
Background: Noninvasive, practical, and convenient means of detection for the prediction of liver fibrosis and cirrhosis in China are greatly needed.
Aim: To develop a precise noninvasive test to stage liver fibrosis and cirrhosis.
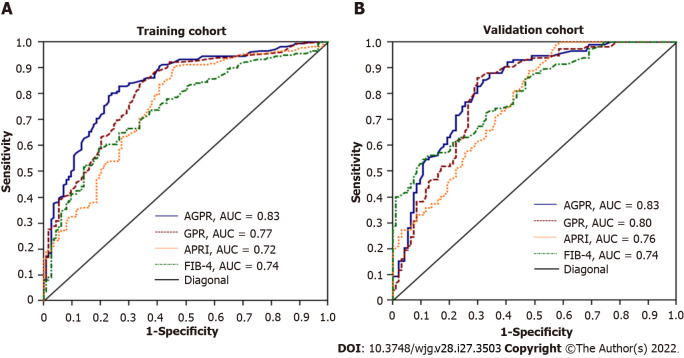
Methods: With liver biopsy as the gold standard, we established a new index, [alkaline phosphatase (U/L) + gamma-glutamyl transpeptidase (U/L)/platelet (109/L) (AGPR)], to predict liver fibrosis and cirrhosis. In addition, we compared the area under the receiver operating characteristic curve (AUROC) of AGPR, gamma-glutamyl transpeptidase to platelet ratio, aspartate transaminase to platelet ratio index, and FIB-4 and evaluated the accuracy of these routine laboratory indices in predicting liver fibrosis and cirrhosis.
Results: Correlation analysis revealed a significant positive correlation between AGPR and liver fibrosis stage (P < 0.001). In the training cohort, the AUROC of AGPR was 0.83 (95%CI: 0.78-0.87) for predicting fibrosis (≥ F2), 0.84 (95%CI: 0.79-0.88) for predicting extensive fibrosis (≥ F3), and 0.87 (95%CI: 0.83-0.91) for predicting cirrhosis (F4). In the validation cohort, the AUROCs of AGPR to predict ≥ F2, ≥ F3 and F4 were 0.83 (95%CI: 0.77-0.88), 0.83 (95%CI: 0.77-0.89), and 0.84 (95%CI: 0.78-0.89), respectively.
Conclusion: The AGPR index should become a new, simple, accurate, and noninvasive marker to predict liver fibrosis and cirrhosis in chronic hepatitis B patients.
Keywords: Chronic hepatitis B; Cirrhosis; Fibrosis; Liver; Novel noninvasive marker; Prediction.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: There are no conflicts of interest to report.
Figures

References
-
- Park YE, Kim BK, Park JY, Kim DY, Ahn SH, Han KH, Han S, Jeon MY, Heo JY, Song K, Kim SU. Gamma-glutamyl transpeptidase-to-platelet ratio is an independent predictor of hepatitis B virus-related liver cancer. J Gastroenterol Hepatol. 2017;32:1221–1229. - PubMed
-
- Friedman LS. Controversies in liver biopsy: who, where, when, how, why? Curr Gastroenterol Rep. 2004;6:30–36. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
