

Outcomes of enhanced recovery after surgery in lung cancer: A systematic review and meta-analysis
- PMID: 36158708
- PMCID: PMC9500517
- DOI: 10.1016/j.apjon.2022.100110
Outcomes of enhanced recovery after surgery in lung cancer: A systematic review and meta-analysis
Abstract
Objective: To assess the effect of ERAS on clinical prognosis in perioperative patients following lung cancer surgery.
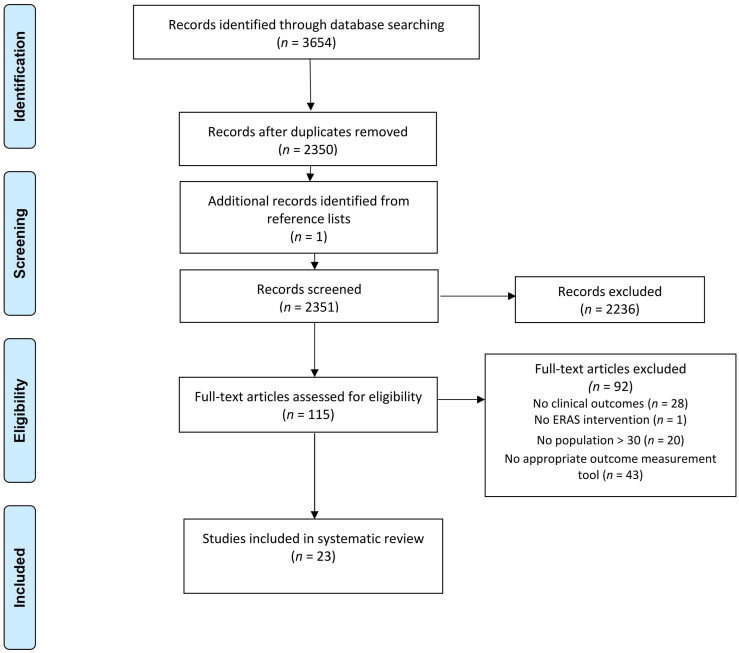
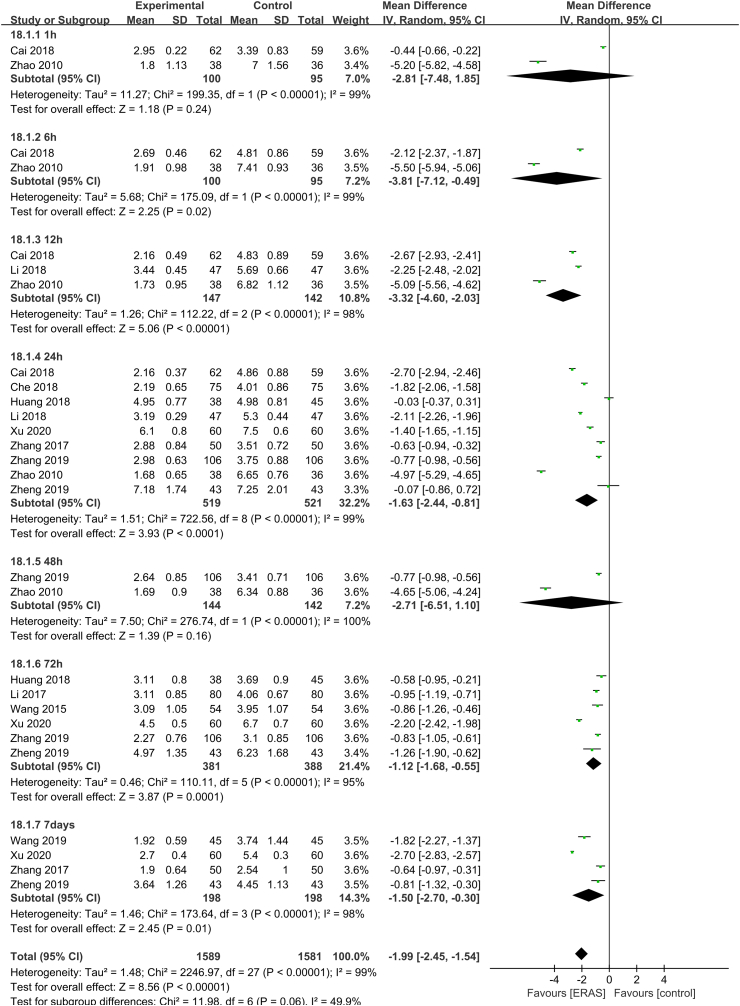
Methods: PubMed, Web of Science, MEDLINE, EMBASE, and other databases were systematically searched from inception to December 2021. Randomized controlled trials and peer-reviewed cohort studies on the use of ERAS in lung cancer surgery patients were included. Primary outcomes comprised visual analog scale scores after treatment and quality of life. Secondary outcomes comprised complication rate, function-related outcomes (chest tube indwelling time and first ambulation), and length of stay. Statistical analysis was performed using RevMan 5.4.1 software.
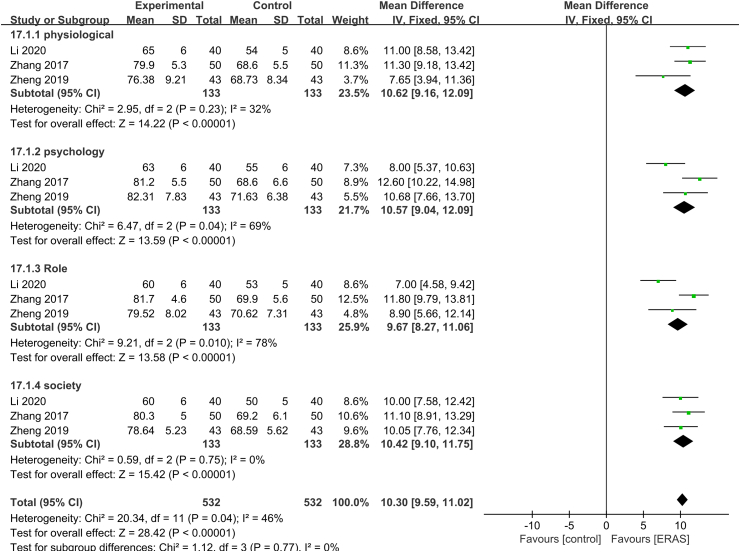
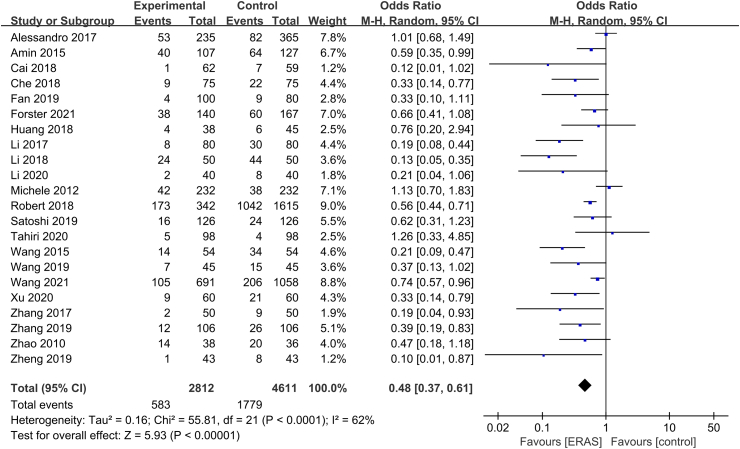
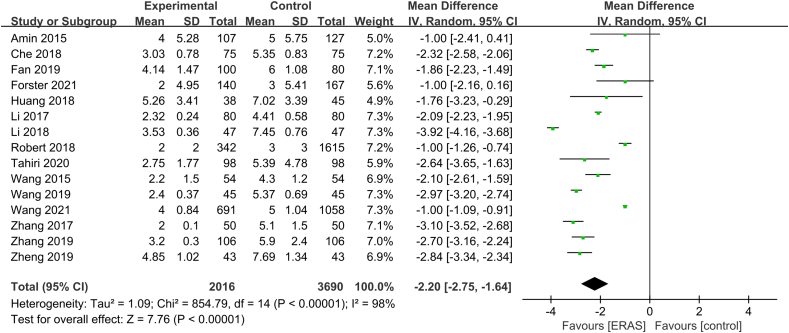
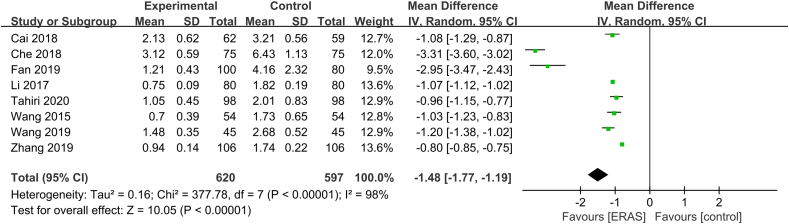
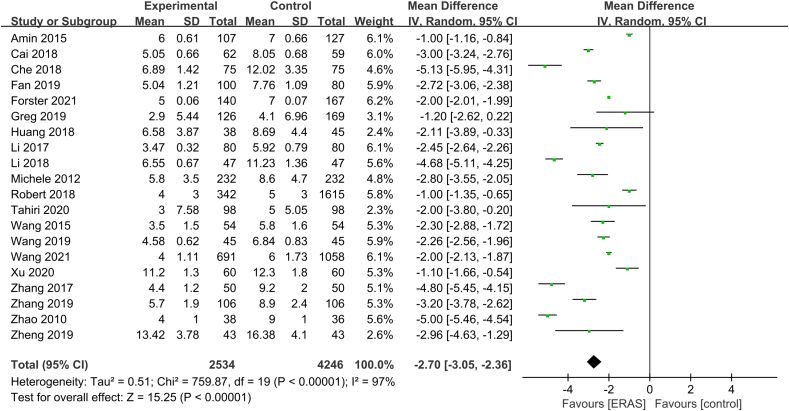
Results: Finally, 23 studies were included (12 cohort studies and 11 randomized controlled trials) with a total of 8094 patients. Meta-analysis showed that ERAS significantly reduced visual analog scale scores (mean difference [MD] = -1.99, 95% confidence interval [CI] = -2.45, -1.54, P < 0.01), reduced the incidence of complications (odds ratio = 0.48, 95% CI = 0.37, 0.61, P < 0.01), shortened chest tube indwelling time (MD = -2.20, 95% CI = -2.75, -1.64, P < 0.01), accelerated first ambulation (MD = -1.48, 95% CI = -1.77, -1.19, P < 0.01), shortened length of stay (MD = -2.70, 95% CI = -3.05, -2.36, P < 0.01), and improved quality of life (MD = 10.3, 95% CI = 9.59, 11.02, P < 0.01).
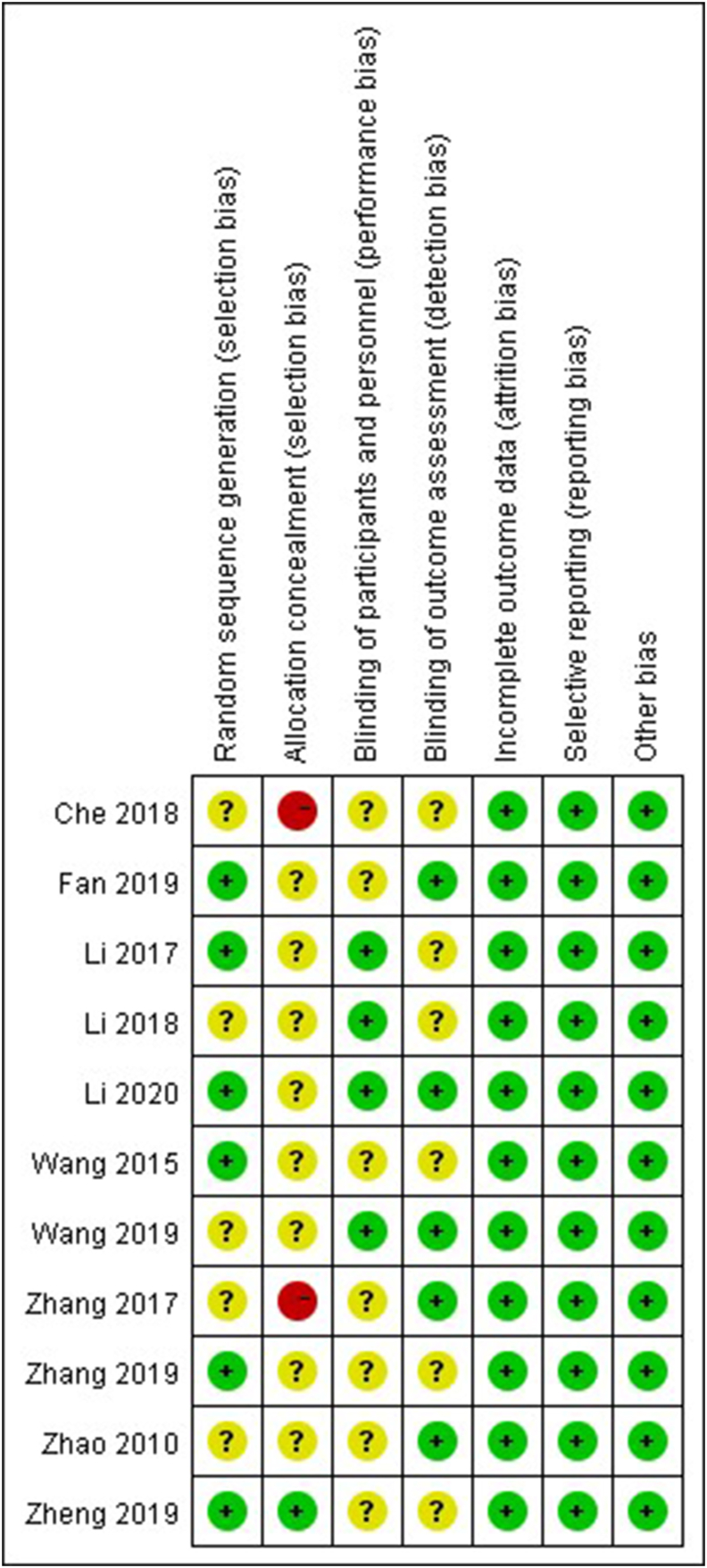
Conclusions: ERAS can accelerate postoperative recovery and improve quality of life. These findings support the use of ERAS as a standard of care for lung cancer surgery patients. However, the evidence quality was moderate and there were significant differences among studies. More high-quality studies incorporating relevant outcomes are needed for confirmation.
Keywords: Enhanced recovery after surgery; Meta-analysis; lung cancer; perioperative care; systematic review.
© 2022 The Author(s).
Figures
Similar articles
-
Enhanced recovery after surgery (ERAS) versus standard recovery for elective gastric cancer surgery: A meta-analysis of randomized controlled trials.Surg Oncol. 2020 Mar;32:75-87. doi: 10.1016/j.suronc.2019.11.004. Epub 2019 Nov 25. Surg Oncol. 2020. PMID: 31786352
-
Effect of the enhanced recovery after surgery protocol on recovery after laparoscopic myomectomy: a systematic review and meta-analysis.Gland Surg. 2022 May;11(5):837-846. doi: 10.21037/gs-22-168. Gland Surg. 2022. PMID: 35694088 Free PMC article.
-
The effect of the enhanced recovery after surgery program on lung cancer surgery: a systematic review and meta-analysis.J Thorac Dis. 2021 Jun;13(6):3566-3586. doi: 10.21037/jtd-21-433. J Thorac Dis. 2021. PMID: 34277051 Free PMC article.
-
[Meta-analysis on safety of application of enhanced recovery after surgery to laparoscopic bariatric surgery].Zhonghua Wei Chang Wai Ke Za Zhi. 2018 Oct 25;21(10):1167-1174. Zhonghua Wei Chang Wai Ke Za Zhi. 2018. PMID: 30370517 Chinese.
-
Paravertebral anaesthesia with or without sedation versus general anaesthesia for women undergoing breast cancer surgery.Cochrane Database Syst Rev. 2021 Feb 25;2(2):CD012968. doi: 10.1002/14651858.CD012968.pub2. Cochrane Database Syst Rev. 2021. PMID: 33629404 Free PMC article.
Cited by
-
Effects of accelerated rehabilitation surgical care on the surgical site wound infection and postoperative complications in patients of lung cancer: A meta-analysis.Int Wound J. 2024 Apr;21(4):e14551. doi: 10.1111/iwj.14551. Epub 2023 Dec 11. Int Wound J. 2024. Retraction in: Int Wound J. 2024 Dec;21(12):e70166. doi: 10.1111/iwj.70166. PMID: 38084011 Free PMC article. Retracted.
-
Impact of Remote Symptom Management on Exercise Adherence After Video-Assisted Thoracic Surgery for Lung Cancer in a Tertiary Hospital in China: Protocol for a Prospective Randomized Controlled Trial.JMIR Res Protoc. 2025 Jan 1;14:e60420. doi: 10.2196/60420. JMIR Res Protoc. 2025. PMID: 39610048 Free PMC article.
-
Orthostatic intolerance during early mobilization following thoracoscopic lung resection: a prospective observational study.BMC Surg. 2024 Sep 16;24(1):265. doi: 10.1186/s12893-024-02556-3. BMC Surg. 2024. PMID: 39285467 Free PMC article.
-
Current Status and Influencing Factors of Readiness for Hospital Discharge of Lung Cancer Patients Receiving ERAS-Guided Postoperative Management.Cancer Control. 2024 Jan-Dec;31:10732748241287011. doi: 10.1177/10732748241287011. Cancer Control. 2024. PMID: 39334516 Free PMC article.
-
Priorities and strategy for the implementation of enhanced recovery after surgery (ERAS) in thoracic surgery.J Thorac Dis. 2024 Jul 30;16(7):4165-4173. doi: 10.21037/jtd-23-1866. Epub 2024 Jun 28. J Thorac Dis. 2024. PMID: 39144305 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
