

Outcomes in Emergency Department Patients with Dyspnea versus Chest Pain: A Retrospective Consecutive Cohort Study
- PMID: 36158766
- PMCID: PMC9507768
- DOI: 10.1155/2022/4031684
Outcomes in Emergency Department Patients with Dyspnea versus Chest Pain: A Retrospective Consecutive Cohort Study
Abstract
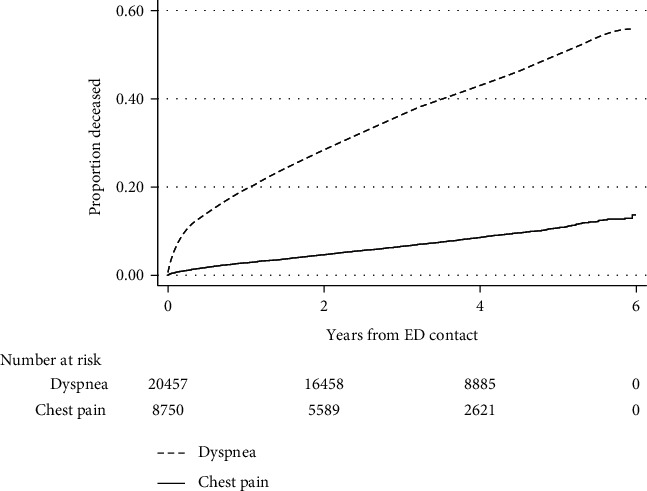
Dyspnea and chest pain are major and important causes of contact at the emergency department (ED). Dyspnea is associated with high morbidity and mortality, but data on characteristics and outcomes compared with chest pain in the ED are limited. This was a retrospective cohort study of consecutive patients with contact causes of dyspnea or chest pain at two Swedish EDs from 2010 to 2014. Hospital admittance, ED revisits, and mortality were analyzed using multivariable regression models, adjusted for ED and markers of disease severity (age, sex, centre, Charlson comorbidity index, c-reactive protein, troponin T, and arrival by ambulance). 29,291 patients (mean age 58.3 years; 48.9% women) with dyspnea (n = 8,812) or chest pain (n = 20,479) were included. Dyspnea patients were older than patients with chest pain (64 vs. 56 years, p < 0.001) and had more comorbidity and higher average blood troponin T and c-reactive protein levels. Dyspnea patients also had higher hospitalization rates (48% vs. 30%; adjOR (95% CI) 2.1-2.3), including the intensive care unit (1.4% vs. 0.1%; adjOR 6.9-15.9), and more ED revisits (11% vs. 7%; adjOR 1.2-1.7) in 30 days. Dyspnea patients had five-fold increased mortality compared to those with chest pain; hazard ratio (HR) 5.1 (4.8-5.4), adjusted for markers of disease severity, the mortality was two-fold higher, HR 2.2 (2.0-2.4). Compared with chest pain patients, ED dyspnea patients are older, have more comorbidity, and have worse outcomes in terms of hospitalization, morbidity, and mortality.
Copyright © 2022 Erik Jemt et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Elderly patients with non-specific complaints at the emergency department have a high risk for admission and 30-days mortality.BMC Geriatr. 2024 Jan 3;24(1):5. doi: 10.1186/s12877-023-04621-7. BMC Geriatr. 2024. PMID: 38172691 Free PMC article.
-
Associations Between Crowding and Ten-Day Mortality Among Patients Allocated Lower Triage Acuity Levels Without Need of Acute Hospital Care on Departure From the Emergency Department.Ann Emerg Med. 2019 Sep;74(3):345-356. doi: 10.1016/j.annemergmed.2019.04.012. Epub 2019 Jun 20. Ann Emerg Med. 2019. PMID: 31229391
-
Risk of revisits to the emergency department in admitted versus discharged patients with chest pain but without myocardial infarction in relation to high-sensitivity cardiac troponin T levels.Int J Cardiol. 2016 Jan 15;203:341-6. doi: 10.1016/j.ijcard.2015.10.170. Epub 2015 Oct 21. Int J Cardiol. 2016. PMID: 26529084
-
The association of biological sex and long-term outcomes in patients with acute dyspnea at the emergency department.Eur J Emerg Med. 2022 Jun 1;29(3):195-203. doi: 10.1097/MEJ.0000000000000899. Epub 2021 Dec 22. Eur J Emerg Med. 2022. PMID: 34954724
-
Seasonal variations of patients presenting dyspnea to emergency departments in Europe: Results from the EURODEM Study.Turk J Med Sci. 2020 Dec 17;50(8):1879-1886. doi: 10.3906/sag-2002-221. Turk J Med Sci. 2020. PMID: 32562519 Free PMC article.
Cited by
-
A novel interpretable deep learning model for diagnosis in emergency department dyspnoea patients based on complete data from an entire health care system.PLoS One. 2024 Dec 27;19(12):e0311081. doi: 10.1371/journal.pone.0311081. eCollection 2024. PLoS One. 2024. PMID: 39729465 Free PMC article.
-
Characteristics of patients who return to the emergency department after an observation-unit assessment.Clin Exp Emerg Med. 2024 Dec;11(4):349-357. doi: 10.15441/ceem.24.192. Epub 2024 May 23. Clin Exp Emerg Med. 2024. PMID: 38778494 Free PMC article.
-
Associations between Chest Pain, Diagnosis, and Clinical Outcome in Patients Hospitalized with Acute Dyspnea: Data from the ACE 2 Study.Cardiology. 2025;150(3):233-242. doi: 10.1159/000541897. Epub 2024 Oct 16. Cardiology. 2025. PMID: 39413740 Free PMC article.
-
Prognosis of patients with nonspecific electrocardiogram findings in a Tanzanian emergency department.Am Heart J. 2025 Mar;281:10-19. doi: 10.1016/j.ahj.2024.11.006. Epub 2024 Dec 19. Am Heart J. 2025. PMID: 39577681
References
-
- Langlo N. M., Orvik A. B., Dale J., Uleberg O., Bjornsen L. P. The acute sick and injured patients: an overview of the emergency department patient population at a Norwegian University Hospital Emergency Department. European Journal of Emergency Medicine . 2014;21(3):175–180. doi: 10.1097/mej.0b013e3283629c18. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
