

Thin filament cardiomyopathies: A review of genetics, disease mechanisms, and emerging therapeutics
- PMID: 36158814
- PMCID: PMC9489950
- DOI: 10.3389/fcvm.2022.972301
Thin filament cardiomyopathies: A review of genetics, disease mechanisms, and emerging therapeutics
Abstract
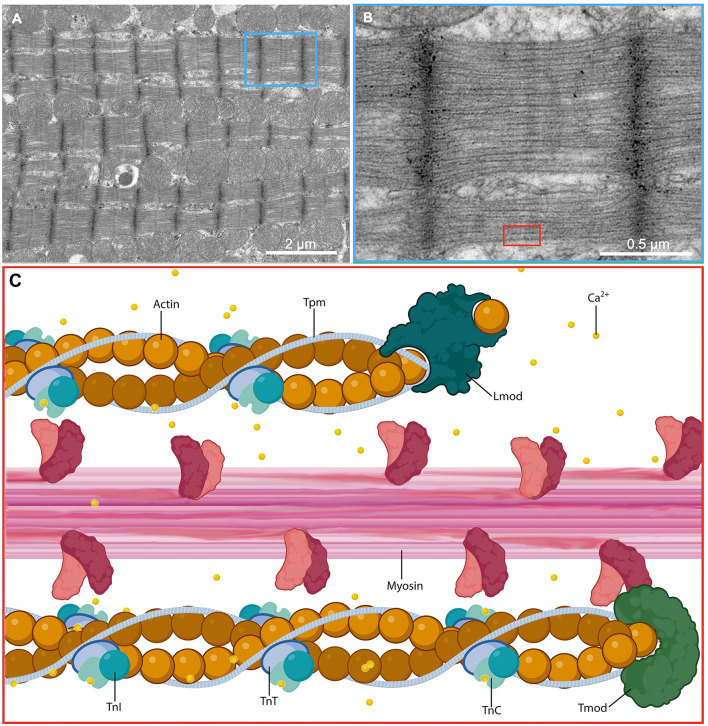
All muscle contraction occurs due to the cyclical interaction between sarcomeric thin and thick filament proteins within the myocyte. The thin filament consists of the proteins actin, tropomyosin, Troponin C, Troponin I, and Troponin T. Mutations in these proteins can result in various forms of cardiomyopathy, including hypertrophic, restrictive, and dilated phenotypes and account for as many as 30% of all cases of inherited cardiomyopathy. There is significant evidence that thin filament mutations contribute to dysregulation of Ca2+ within the sarcomere and may have a distinct pathomechanism of disease from cardiomyopathy associated with thick filament mutations. A number of distinct clinical findings appear to be correlated with thin-filament mutations: greater degrees of restrictive cardiomyopathy and relatively less left ventricular (LV) hypertrophy and LV outflow tract obstruction than that seen with thick filament mutations, increased morbidity associated with heart failure, increased arrhythmia burden and potentially higher mortality. Most therapies that improve outcomes in heart failure blunt the neurohormonal pathways involved in cardiac remodeling, while most therapies for hypertrophic cardiomyopathy involve use of negative inotropes to reduce LV hypertrophy or septal reduction therapies to reduce LV outflow tract obstruction. None of these therapies directly address the underlying sarcomeric dysfunction associated with thin-filament mutations. With mounting evidence that thin filament cardiomyopathies occur through a distinct mechanism, there is need for therapies targeting the unique, underlying mechanisms tailored for each patient depending on a given mutation.
Keywords: ACTC1; TNNC1; TNNI3; TNNT2; TPM1; cardiomyopathy; thin filament.
Copyright © 2022 Keyt, Duran, Bui, Chen, Miyamoto, Silva Enciso, Tardiff and Adler.
Conflict of interest statement
JD reports personal fees from Lexeo during the conduct of the review. EA reports personal fees from Abiomed, Novartis, Abbott, non-financial support from Astra Zeneca, personal fees from Ionis Pharmaceuticals, Sana Biotechnology, Medtronic, other from Rocket Pharmaceuticals, Papillon Therapeutics, ResQ Pharmaceuticals, personal fees from Lexeo Pharmaceuticals, Cytokinetics, Endotronics, and during the conduct of the review. MM was employed by Providence Health. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, et al. . Contemporary definitions and classification of the cardiomyopathies: an American heart association scientific statement from the council on clinical cardiology, heart failure and transplantation committee; quality of care and outcomes research and functional genomics and translational biology interdisciplinary working groups; and council on epidemiology and prevention. Circulation. (2006) 113:1807–16. 10.1161/CIRCULATIONAHA.106.174287 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous