

doi: 10.5826/dpc.1203a123.
eCollection 2022 Jul.
Dermoscopy for Acral Melanocytic Lesions: Revision of the 3-step Algorithm and Refined Definition of the Regular and Irregular Fibrillar Pattern
Affiliations
- PMID: 36159128
- PMCID: PMC9464531
- DOI: 10.5826/dpc.1203a123
Item in Clipboard
Dermoscopy for Acral Melanocytic Lesions: Revision of the 3-step Algorithm and Refined Definition of the Regular and Irregular Fibrillar Pattern
Dermatol Pract Concept.
.
No abstract available
Conflict of interest statement
Competing interests: None.
Figures

The re-revised 3-step algorithm for the management of melanocytic lesions on acral volar skin. The main targets of this algorithm are macular/patch lesions seen in adults. Apparently congenital lesions and nodular lesions are excluded from the evaluation.

Regular fibrillar pattern of acral nevus (dermoscopy with the furrow ink test). (A) The fibrils constituting the pattern are regular in color, thickness and distribution. All the endpoints of the fibrils line up on the sulci of the skin markings. The pattern changes to the parallel furrow pattern in the lower portion. (B) The oblique dermoscopy reveals that this is originally the parallel furrow pattern.

Regular fibrillar pattern of acral nevus (dermoscopy with the furrow ink test). (A) The fibrils constituting the pattern are regular in color, thickness and distribution. All the endpoints of the fibrils line up on the sulci of the skin markings. The pattern changes to the parallel furrow pattern in the lower portion. (B) The oblique dermoscopy reveals that this is originally the parallel furrow pattern.

Irregular fibrillar pattern of acral melanoma in situ. This lesion of the multicomponent pattern is mostly composed of fibrils and can be regarded as the irregular FP by our definition, ie, the fibrils constituting the pattern are irregular in color, thickness and distribution, and their endpoints do not line up on the sulci of the skin markings. (A) Transition to the parallel ridge pattern is detected in the right lower portion. The negative fibrillar pattern (whitish rods arranged in a parallel fashion) are detected in the left area, which is well recognized in (B), an image of higher magnification corresponding to the square area in (A). (B) Arrows indicate some of the whitish rods.

Irregular fibrillar pattern of acral melanoma in situ. This lesion of the multicomponent pattern is mostly composed of fibrils and can be regarded as the irregular FP by our definition, ie, the fibrils constituting the pattern are irregular in color, thickness and distribution, and their endpoints do not line up on the sulci of the skin markings. (A) Transition to the parallel ridge pattern is detected in the right lower portion. The negative fibrillar pattern (whitish rods arranged in a parallel fashion) are detected in the left area, which is well recognized in (B), an image of higher magnification corresponding to the square area in (A). (B) Arrows indicate some of the whitish rods.
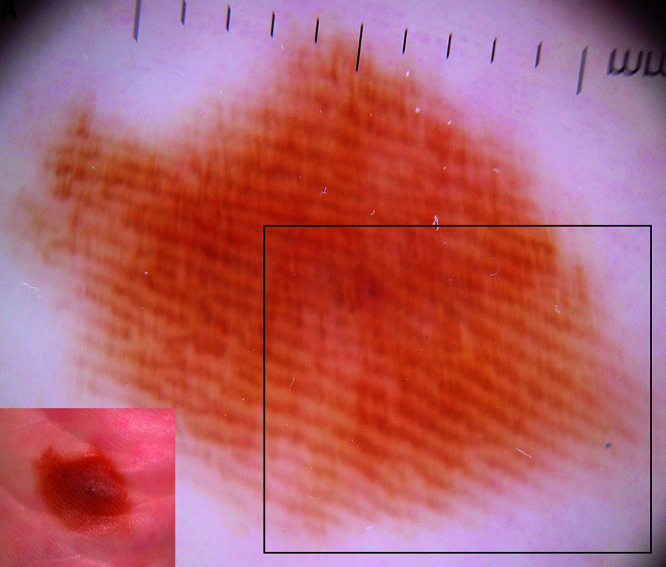
“Regular” fibrillar pattern seen in acral melanoma in situ (A, inset: clinical features: a brown patch, 13.5 × 10.5 mm in size, seen on the sole of a 78-year-old woman). (A) The very thin fibrils constituting this fibrillar pattern are evenly arranged and regular in color and thickness. (B) the square area in (A). The furrow ink test reveals that the sulci of the skin markings, indicated with arrows, are spared from the fibrillar pigmentation. (C, D) Histopathological features. (D) corresponds to the square area in (C). The thick cornified layer is obliquely arranged, as indicated with arrows in (C). The increased number of melanocytes are mainly detected in the crista profunda intermedia indicated with asterisks in (C) and their nuclei are large and hyperchromatic as seen in (D), confirming this is acral melanoma in situ. (Note: FISH analysis of this lesion revealed amplification of cyclin D1.)

“Regular” fibrillar pattern seen in acral melanoma in situ (A, inset: clinical features: a brown patch, 13.5 × 10.5 mm in size, seen on the sole of a 78-year-old woman). (A) The very thin fibrils constituting this fibrillar pattern are evenly arranged and regular in color and thickness. (B) the square area in (A). The furrow ink test reveals that the sulci of the skin markings, indicated with arrows, are spared from the fibrillar pigmentation. (C, D) Histopathological features. (D) corresponds to the square area in (C). The thick cornified layer is obliquely arranged, as indicated with arrows in (C). The increased number of melanocytes are mainly detected in the crista profunda intermedia indicated with asterisks in (C) and their nuclei are large and hyperchromatic as seen in (D), confirming this is acral melanoma in situ. (Note: FISH analysis of this lesion revealed amplification of cyclin D1.)

“Regular” fibrillar pattern seen in acral melanoma in situ (A, inset: clinical features: a brown patch, 13.5 × 10.5 mm in size, seen on the sole of a 78-year-old woman). (A) The very thin fibrils constituting this fibrillar pattern are evenly arranged and regular in color and thickness. (B) the square area in (A). The furrow ink test reveals that the sulci of the skin markings, indicated with arrows, are spared from the fibrillar pigmentation. (C, D) Histopathological features. (D) corresponds to the square area in (C). The thick cornified layer is obliquely arranged, as indicated with arrows in (C). The increased number of melanocytes are mainly detected in the crista profunda intermedia indicated with asterisks in (C) and their nuclei are large and hyperchromatic as seen in (D), confirming this is acral melanoma in situ. (Note: FISH analysis of this lesion revealed amplification of cyclin D1.)

“Regular” fibrillar pattern seen in acral melanoma in situ (A, inset: clinical features: a brown patch, 13.5 × 10.5 mm in size, seen on the sole of a 78-year-old woman). (A) The very thin fibrils constituting this fibrillar pattern are evenly arranged and regular in color and thickness. (B) the square area in (A). The furrow ink test reveals that the sulci of the skin markings, indicated with arrows, are spared from the fibrillar pigmentation. (C, D) Histopathological features. (D) corresponds to the square area in (C). The thick cornified layer is obliquely arranged, as indicated with arrows in (C). The increased number of melanocytes are mainly detected in the crista profunda intermedia indicated with asterisks in (C) and their nuclei are large and hyperchromatic as seen in (D), confirming this is acral melanoma in situ. (Note: FISH analysis of this lesion revealed amplification of cyclin D1.)

Regular fibrillar pattern composed of thick fibrils. A small brown macule, 4 mm in diameter, seen on the sole of a 38-year-old woman. This fibrillar pattern is composed of regularly arranged thick fibrils, of which endpoints line up on the sulci of the skin markings. Although the color density of the fibrils is somewhat different within the lesion, the color distribution is mostly symmetric, indicating this is the regular FP. From these findings, we can certainly diagnose this lesion as acral nevus. Note: These thick fibrils indicate that melanocytes in the epidermis are not distributed as solitary units but arranged mostly in larger nests, which is an important histopathologic clue to benign nevus of a small size such as this one (4mm).
Similar articles
-
[Dermoscopic pattern analysis of acral melanocytic nevi].Przegl Lek. 2013;70(11):911-5. Przegl Lek. 2013. PMID: 24697028 Polish.
-
Educational and practice gaps in the management of volar melanocytic lesions.J Eur Acad Dermatol Venereol. 2018 Sep;32(9):1450-1455. doi: 10.1111/jdv.14712. Epub 2017 Dec 18. J Eur Acad Dermatol Venereol. 2018. PMID: 29178552 Free PMC article.
-
Age and Anatomical Location-Related Dermoscopic Patterns of 210 Acral Melanocytic Nevi in a Turkish Population.J Cutan Med Surg. 2017 Sep/Oct;21(5):388-394. doi: 10.1177/1203475417712496. Epub 2017 Jun 1. J Cutan Med Surg. 2017. PMID: 28565919
-
Dermoscopic patterns of acral melanocytic lesions in skin of color.Cutis. 2019 May;103(5):274-276. Cutis. 2019. PMID: 31233579 Review.
-
Key points in dermoscopic differentiation between early acral melanoma and acral nevus.J Dermatol. 2011 Jan;38(1):25-34. doi: 10.1111/j.1346-8138.2010.01174.x. J Dermatol. 2011. PMID: 21175752 Review.
Cited by
-
Acral lentiginous melanoma in situ on the palm with a diffuse parallel furrow pattern.JAAD Case Rep. 2024 Oct 16;54:66-68. doi: 10.1016/j.jdcr.2024.09.025. eCollection 2024 Dec. JAAD Case Rep. 2024. PMID: 39654852 Free PMC article. No abstract available.
-
Pattern Analysis of Benign and Malignant Atypical Melanocytic Skin Lesions of Palms and Soles: Variations of Dermoscopic Features According to Anatomic Site and Personal Experience.Life (Basel). 2024 May 22;14(6):659. doi: 10.3390/life14060659. Life (Basel). 2024. PMID: 38929643 Free PMC article.
-
Validation of a Dermatoscopy-Based Algorithm for the Diagnosis of Acral Melanoma.Dermatology. 2024;240(5-6):793-802. doi: 10.1159/000541591. Epub 2024 Oct 5. Dermatology. 2024. PMID: 39369689 Free PMC article.
References
LinkOut - more resources
Full Text Sources