

Facial Dermatoses in Patients With Blepharitis: a Cross-sectional Prospective Analysis
- PMID: 36159148
- PMCID: PMC9464537
- DOI: 10.5826/dpc.1203a113
Facial Dermatoses in Patients With Blepharitis: a Cross-sectional Prospective Analysis
Abstract
Introduction: The relationship between facial dermatoses and blepharitis has been known for a long time.
Objectives: We aimed to investigate the frequency of accompanying facial dermatoses in patients with blepharitis and their relationship with the severity of blepharitis.
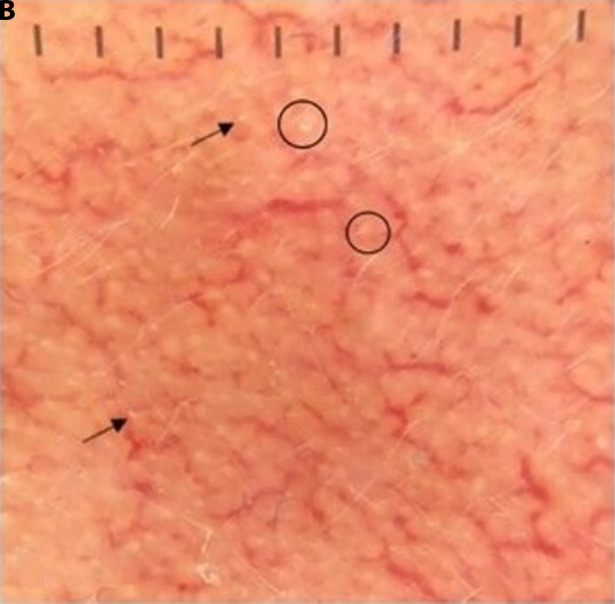
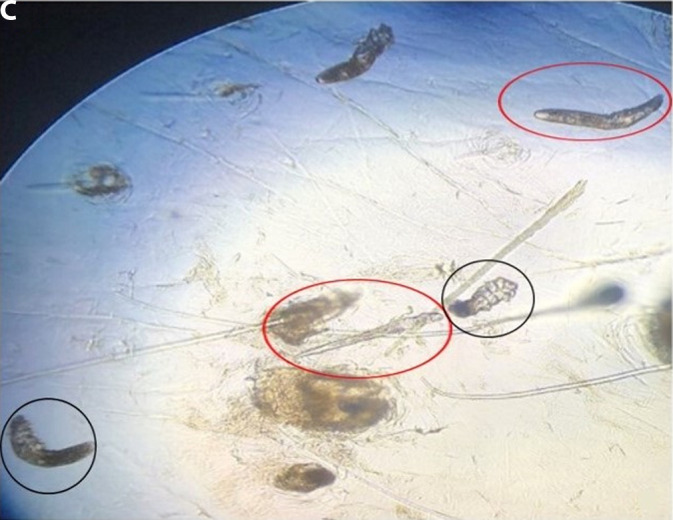
Methods: In this cross-sectional study, 95 patients with blepharitis were examined for attending facial dermatoses. The type of blepharitis, the severity of blepharitis, and the degree of dry eye were determined in the patients. Dermoscopic and microscopic examinations were used in the diagnosis of facial dermatoses. The history of allergic rhinitis was questioned because Demodex species frequently accompany blepharitis, facial dermatoses, and allergic rhinitis patients. Mann-Whitney U test was used compare 2 independent groups. In comparing categorical variables, Pearson chi-Squared, Fishere Exact, and Fisher-Freeman-Holton tests were used.
Results: At least 1 facial dermatosis was detected in 84.2% patients, and we did not see any facial dermatosis in 15.8% ones. No patients had acne, which is one of the most common facial dermatoses. The most common facial dermatosis detected in our patients was facial demodicosis (57.9%). It was followed by seborrheic dermatitis (22.1%) and rosacea (12.6%), respectively. In addition, 2.1% of the patients had atopic eyelid dermatitis, 23.2% had a history of allergic rhinitis, and 63.2% had ocular demodicosis.
Conclusions: It is essential to perform dermatological examinations of all patients with blepharitis in terms of accompanying facial dermatoses and their early diagnosis.
Keywords: blepharitis; demodicosis; facial dermatoses; rosacea; seborrheic dermatitis.
©2022 Güder et al.
Conflict of interest statement
Competing interests: None.
Figures














Similar articles
-
Increased frequency of Demodex blepharitis in rosacea and facial demodicosis patients.J Cosmet Dermatol. 2020 May;19(5):1260-1265. doi: 10.1111/jocd.13150. Epub 2019 Sep 25. J Cosmet Dermatol. 2020. PMID: 31553138
-
Demodex folliculorum infestations in common facial dermatoses: acne vulgaris, rosacea, seborrheic dermatitis.An Bras Dermatol. 2020 Mar-Apr;95(2):187-193. doi: 10.1016/j.abd.2019.08.023. Epub 2020 Feb 12. An Bras Dermatol. 2020. PMID: 32113677 Free PMC article.
-
Beyond the Surface: Understanding Demodex and Its Link to Blepharitis and Facial Dermatoses.Clin Ophthalmol. 2024 Jun 24;18:1801-1810. doi: 10.2147/OPTH.S440199. eCollection 2024. Clin Ophthalmol. 2024. PMID: 38948346 Free PMC article. Review.
-
Palpebral and facial skin infestation by Demodex folliculorum.Cont Lens Anterior Eye. 2020 Apr;43(2):115-122. doi: 10.1016/j.clae.2019.09.001. Epub 2019 Sep 25. Cont Lens Anterior Eye. 2020. PMID: 31563449
-
Demodicosis in Different Age Groups and Alternative Treatment Options-A Review.J Clin Med. 2023 Feb 19;12(4):1649. doi: 10.3390/jcm12041649. J Clin Med. 2023. PMID: 36836184 Free PMC article. Review.
Cited by
-
Ocular Manifestations in Seborrheic Dermatitis Epidemiology, Clinical Features, and Management: A Comprehensive Review.Cureus. 2024 Sep 27;16(9):e70335. doi: 10.7759/cureus.70335. eCollection 2024 Sep. Cureus. 2024. PMID: 39463532 Free PMC article. Review.
-
Preferred practice patterns and review on rosacea.Indian J Ophthalmol. 2023 Apr;71(4):1382-1390. doi: 10.4103/IJO.IJO_2983_22. Indian J Ophthalmol. 2023. Retraction in: Indian J Ophthalmol. 2023 Sep;71(9):3272. doi: 10.4103/0301-4738.383879. PMID: 37026270 Free PMC article. Retracted. Review.
-
Uncommon Blepharitis.J Clin Med. 2024 Jan 25;13(3):710. doi: 10.3390/jcm13030710. J Clin Med. 2024. PMID: 38337403 Free PMC article.
-
Evaluation of Meibography Findings and Ocular Surface Parameters in Children with Atopic Dermatitis Without Eye Complaints.Children (Basel). 2025 Jan 27;12(2):150. doi: 10.3390/children12020150. Children (Basel). 2025. PMID: 40003252 Free PMC article.
References
-
- Bron AJ, Tiffany JM. The Evolution of Lid Margin Changes in Blepharitis. In: Lass JH, editor. Advances in Corneal Research: Selected Transactions of the World Congress on the Cornea IV. Boston, MA: Springer US; 1997. pp. 3–18.
-
- Hsu JI, Pflugfelder SC, Kim SJ. Ocular complications of atopic dermatitis. Cutis. 2019;104(3):189–193. - PubMed
LinkOut - more resources
Full Text Sources