

Challenges of Differential Diagnosis Between Primary Hyperparathyroidism and Bone Metastases of Breast Cancer
- PMID: 36159181
- PMCID: PMC9493671
- DOI: 10.1177/11795476221125136
Challenges of Differential Diagnosis Between Primary Hyperparathyroidism and Bone Metastases of Breast Cancer
Abstract
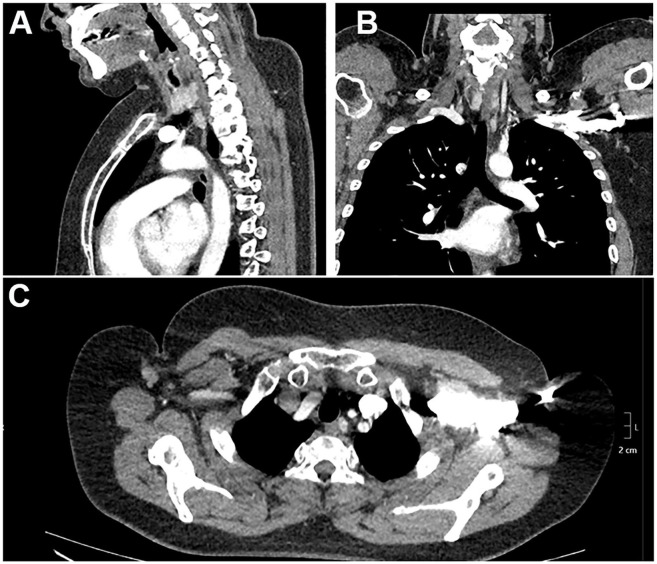
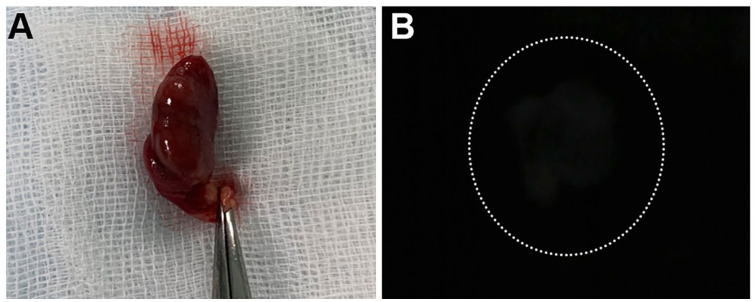
Breast cancer might be complicated by distant metastases accompanied by hypercalcemia, but hyperparathyroidism is not commonly considered in the differential diagnosis. We present a case of 38 years old female patient who was diagnosed with ductal breast carcinoma. Eight months after the initial diagnosis the patient was diagnosed with distant bone metastases. However, this diagnosis was reconsidered at follow up, because we identified elevation of PTH 137.2 pg/ml, Ca2+ 1.19 mmol/l, albumin corrected calcium 2.42 mmol/l, 25(OH)D 39.4 nmol/l, indicating hyperparathyroidism. Scintigraphy with 99mTC-sestamibi confirmed parathyroid adenoma. Postoperative histopathology confirmed 1.2 g chief-cell PTA. Two months after the operation both PTH and Ca2+ levels were within the normal ranges. This study emphasizes the importance of considering possible hyperparathyroidism in patients with breast cancer and hypercalcemia. Routine evaluation of PTH is considered as a reasonable test in patients with breast cancer accompanied by bone lesions.
Keywords: Diagnosis; bone demineralization; bone diseases; breast; carcinoma; differential; ductal; endocrine; hyperparathyroidism; pathologic; primary.
© The Author(s) 2022.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



Similar articles
-
Increased prevalence of primary hyperparathyroidism in treated breast cancer.J Endocrinol Invest. 2001 May;24(5):315-20. doi: 10.1007/BF03343867. J Endocrinol Invest. 2001. PMID: 11407650
-
[Changes in mineral metabolism in stage 3, 4, and 5 chronic kidney disease (not on dialysis)].Nefrologia. 2008;28 Suppl 3:67-78. Nefrologia. 2008. PMID: 19018742 Spanish.
-
1alpha(OH)D3 One-alpha-hydroxy-cholecalciferol--an active vitamin D analog. Clinical studies on prophylaxis and treatment of secondary hyperparathyroidism in uremic patients on chronic dialysis.Dan Med Bull. 2008 Nov;55(4):186-210. Dan Med Bull. 2008. PMID: 19232159 Review.
-
Parathyroid adenoma-related hypercalcaemia in breast cancer: a critical diagnosis in clinical oncology.Int J Clin Pract. 2003 Oct;57(8):729-30. Int J Clin Pract. 2003. PMID: 14627187
-
Association of primary hyperparathyroidism and humoral hypercalcemia of malignancy in a patient with clear cell renal carcinoma.Arch Endocrinol Metab. 2015 Feb;59(1):84-8. doi: 10.1590/2359-3997000000015. Arch Endocrinol Metab. 2015. PMID: 25926120 Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
